The Appalachian (F)armacy
|
|
|
- Stephany Harvey
- 5 years ago
- Views:
Transcription
1 The Appalachian (F)armacy An initiative to improve Health outcomes of low income families RHAT 24 th Annual Conference Theme: Rural Healthcare Infrastructure: Vital to Population Health K. Munene Mwirigi, M.P.A., M.S. DrPH(c)
2 Introductions Who do we have here today? Name County/region Occupation/ area of practice Why you come to this presentation
3 Introduction What is Food Insecurity? Why does food quality matter? Food security and health Farmacy Program Recommendations and opportunities for the community Summary
4 Food Insecurity Access by all members of the household at all times to enough food for an active healthy life USDA food insecurity scale when a participant reports 3 or more food-insecure conditions on the survey These includes- Low food security- reports of reduced quality, variety, or desirability of diet Very low food security- multiple indications of disrupted eating patterns and reduced intake Prevalence of food insecurity in the US USDA, Economic Research Service using data from U.S. Department of Commerce, U.S. Census Bureau, Current Population Survey Food Security Supplement.
5 Assessing for Food Insecurity I m going to read you two statements that people have made about their food situation. For each statement, please tell me whether the statement was often true, sometimes true or never true for your household in the last 12 months/ 1 month. 1. We worried whether our food would run out before we got money to buy more. 2. The food that we bought just didn t last, and we didn t have money to get more. A response of often true or sometimes true to either question = positive screen for Food Insecurity
 of the population was food insecure in 2015.")
 Food insecurity and income level 2016 Overall food insecurity")
.")
6 Food Insecurity in TN In Tennessee, 14.5% (about 1 M) of the population was food insecure in (National 12.3%) Food insecurity and income level 2016 Overall food insecurity in TN Counties with highest rates (>20%) Lauderdale, Lake, Hardeman, Haywood, & Shelby Feeding America. (2016). Food insecurity in Tennessee. Retrieved from

7 S O C I A L D E T E R M I N A N T S O F H E A L T H Food insecurity Local economyfarmers and local business Nutrition & Health Knowledge Food Access- Farmers markets & local stores Health & nutrition literacy Case management Improved care Social cohesion and interaction

8 Food insecurity and food quality Food insecure households deploy coping strategies, such as seeking calorically dense and satiating foods that are often nutritionally inadequate. Poor diet quality characterized by high consumption of empty calories and low consumption of fruits and vegetables. Changes in dietary consumption contribute to negative physical and mental outcomes and an increased risk for disease. Holben, D., & Marshall, M. (2017) Position of the Academy of Nutrition and Dietetics: Food Insecurity in the United States. JAND, 117(12).


9 Food insecurity and chronic illness Food insecurity has a bidirectional relationship with chronic illness Report by USDA ERS (2017) using NHIS data Food insecurity is a better predictor of chronic illness than income. Associated with all 10 chronic illnesses vs income with only 3. hypertension, coronary heart disease, hepatitis, stroke, cancer, asthma, diabetes, arthritis, chronic obstructive pulmonary disease, and kidney disease Food security status is also strongly related to the likelihood of chronic disease in general, to the number of chronic conditions reported, and to self-assessed health Berkowitz et al. study (2014) NHIS Data 1 in 3 chronically ill patients were unable to afford food, medications, or both Food Insecure adults more likely to report cost related medication under use Gregory, C. A., & Coleman-Jensen, A. (2017). Food Insecurity, Chronic Disease, and Health Among Working-Age Adults. Berkowitz, S. A., Seligman, H. K., & Choudhry, N. K. (2014). Treat or eat: Food insecurity, cost-related medication underuse, and unmet needs. American Journal of Medicine, 127(4),
10 Chronic illnesses in Tennessee Chronic illnesses now account for 7 of the top 10 causes of death in the US. (2014) Tennessee ranks 45 th on the America s Health Rankings Premature Death (years lost before the age of 75)- about 1 per every 10 deaths (Ranks 43 rd ) Rates in Tennessee Obesity 35% (U.S. 30%) Diabetes 13% (U.S. 10%) Cardiovascular Disease 9% (U.S. 6%) Hypertension 39% (U.S. 31%) United Health Foundation. (2018). America s Health Rankings
11 Food Insecurity- Summary Consequences Affects food quality Associated with medication underuse Associated with poor health outcomes Associated with chronic illness Better predictor of chronic illness than income
12 What are your thoughts? Do you resonate with any of this information? How do you assess for food insecurity in your practice? Do you? What are your thoughts on food insecurity as a risk factor for health?
13 Food Assistance Programs & Healthy Incentives Programs We know all about SNAP, WIC SNAP eligibility is at or below 130% of the federal poverty line- 16,000 per year for 1 person and 33,000 for a household of 4 SNAP lacks restrictions that promote purchase of healthy food items. SNAP participants have lower food quality, lower fruits and vegetable intake and higher empty calorie intake compared to non-snap participants of the same income level Healthy Incentives programs provide incentives to SNAP participants To increase access and encourage purchase of fresh fruits and vegetables. These programs use tokens or vouchers and are mostly found in farmers markets (Nguyen, Shuval, Njike, & Katz, (2014) The Supplemental Nutrition Assistance Program and Dietary Quality Among US Adults: Findings From a Nationally Representative Survey
14 The mechanism of Food Assistance Programs IOM (Institute of Medicine) and NRC (National Research Council) Supplemental Nutrition Assistance Program: Examining the evidence to define benefit adequacy. Washington, DC: The National Academies Press.

15 Why fruits and vegetables? USDA recommendations of about 2 cups per day of fruit and about 3 cups per day of vegetables Very low consumption rates in Tennessee Tennessee ranks 47th in Fruits and veggie consumption Only 7% of the population meets the standard in TN Even lower rates for low income households Nutrient dense & Health outcome Fruits and vegetables provide a variety of nutrients that improve the diet quality and improve health outcomes Access and affordability Fruits and vegetables are expensive and less available in rural areas. The State of Obesity. (2011). Fruits and vegetable consumption.
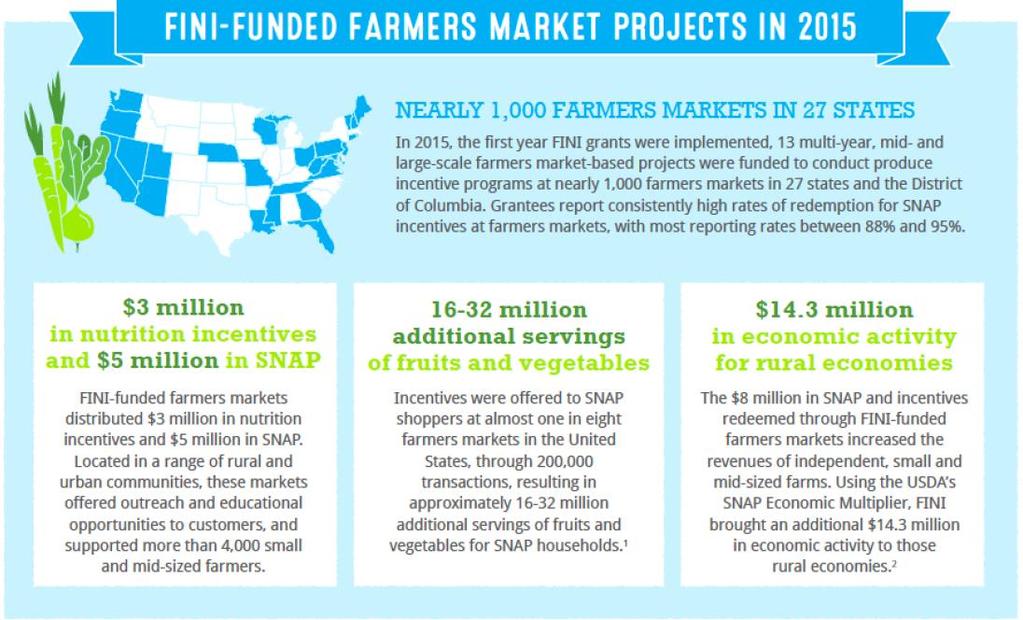
16 Food Insecurity Nutrition Incentives FINI was created under the 2014 Farm Bill Created to develop strategies to improve diet quality of SNAP participants by providing incentives for fresh produce Provide 50/50 match grants to nonprofit and state/local government agencies Programs provide point-of-sale incentives- e.g. coupons Types of grants under FINI FINI pilots: $100,000 over 1 year FINI projects: $500,000 over 4 years FINI large scale projects: $500,000 over 4 years Examples include AARP foundation, Wholesome wave 2018 Farm Bill has not yet been passed. Point-of-sale incentives Currently provide incentives for fresh fruits and vegetables Emphasize utilization of farmers markets Improve the local economy and support local farmers
17
18 Appalachian Farmacy Farmacy initiation Awarded a FINI pilot grant for $100,000 Started in July 2017 July to October- Farmers markets November to March at Food City locations Farmacy Aims: Increase the purchase and consumption of locally produced, fresh fruits and vegetables at Washington County farmer s markets by providing vouchers and nutrition education

")
 Evaluation ETSU College of Public")

 Jonesborough Senior Center")
 Nutrition")
19 Multi-Partner!! Food Insecurity Nutrition Incentives Grant Appalachian Resource Conservation & Development Council (ARC&D) Appalachian Sustainable Development (ASD) Evaluation ETSU College of Public Health Implementation sites Johnson City Community Health Center (CON/JCCHC) Johnson City Senior Center (JCSC) Jonesborough Senior Center (JBSC) 3 Farmers Markets Food City (produce section only) Nutrition classes University of Tennessee Extension (UT) Washington County




20 Appalachian Farmacy Free fruits and vegetable vouchers given as prescriptions Coalition team met monthly Health Assessment JCCHC Senior centers Vouchers Monthly $28- $112 depending on household size Redemption Farmers Market & Food City* Nutrition classes UT Extension


 Thematic analysis Data")
21 Evaluation design Mixed methods approach Quantitative- Survey Baseline Midpoint after Farmer s markets closed 6 months Qualitative Intercept interviews (n=22) 2 focus groups (n=11) Thematic analysis Data analysis on SPSS
22 Survey instruments Survey format Pre-, Mid-,& Post- Similar questions questions Self or staff administered Assessed Fruits & Veggie Intake Types of produce bought Cooking habits Food insecurity Perceptions of fruits and veggies Physical Activity
23 Qualitative Intercept interviews- n=22 Developed Interview scripts 15 minute interviews on perceptions of Farmer s Market and the program About 6 interviews in Spanish Participants approached at the Farmer s Market during check-in Incentive was 5 extra tokens Focus group guides- n=11 (2 sessions) 1 hour session on perceptions of the program, Fruits and vegetables, and health Verbatim note taking





24 Data Management Qualitative Data Separately reviewed transcripts Coded scripts based on guide Jointly Identified recurrent themes Quantitative data Developed a coding sheet Entered information into Excel Entered data into SPSS Descriptive analysis; T-test comparison of means Calculated Food insecurity







25 Baseline Results Variable TN Wash. Farmacy N=134 Adults with some college 67% 59% 43% SNAP eligible food insecure adults 56% 61% 79% Obesity 32% 29% 53% Less than a fruit daily 46% n.d 73% Less than a vegetable daily 25% n.d 72% No physical activity 30% 32% 43% Feeding America (2015) Food insecurity County Health Rankings (2018) The State of Obesity(2011) fruits and vegetable consumption
26 Quantitative Results Recruited over 150 participants Distributed about $50,000 worth of vouchers 60% redeemed at Farmers Markets HH with 4 or more accounted for 33% of the participants and spent 53% of the funds Mean consumption increased (α=.05) Fruits from 4-6 times weekly to 2 times daily Vegetables from 4-6 times weekly to once daily Types of fruits consumed rose from 5 to 8 Types of veggies consumed rose from 6 to 11
27 Monthly redemption Redemption data $8,000 $7,000 $6,000 $5,000 $4,000 $3,000 $2,000 $1,000 Monthly redemption by participants at the farmers market and Food City $- July Aug Sept Oct Nov Dec Jan Feb Mar Total amount $3,535 $5,992 $6,440 $7,070 $3,332 $4,029 $4,382 $2,408 $1,813 60% redeemed at Farmers Markets
28 Qualitative Results I would not have been able to buy fruits and veggies for my kids" Access Helps stretch my dollars things you wouldn t buy otherwise Social cohesion Going to market gets me out of the house and gives me something to look forward to I got some recipes, some hints about how to freeze Perceptions of health works my bowels" Diet is helping. Blood sugar has decreased feeling a whole lot better"
29 Challenges and Gaps Finding partnerships Finding partners to give financial and technical support at the local level Program administration The program requires extensive planning and administration which can be expensive and time consuming May require a fulltime staff Obtaining adequate incentives/funds to meet the needs of the local community Finding adequate funding and partnerships locally. Meeting the 50/50 match requirement
30 Challenges and Gaps Staffing Case management- important for retention and success of the program Clinic verses the senior centers Program administration- centralized management of the program Fulltime program administrator Community engagement- recruitment, education and promotion efforts Community partnerships, advertising Access Transportation services/ management for some participants Local buses, institution buses, Synchronization with other appointments- doctor s visits etc Proximity to farmers markets/ fresh produce Opening farmers markets increasing farmers market days
31 Recommendations Promoting health Although food insecurity didn t improve very much, this indicates that there is a greater need Improving food insecurity, despite limited funding, through nutrition education, community partnerships (farmers, markets, local government, non-profits). Promoting other non-nutrition health programs that improve health- physical activity programs, smoking cessation programs, Case management Participants require accountability, guidance, & reminders to ensure success of the program Participants have unique needs that make it challenging to participate. For example language barrier, transportation, illness, cultural differences Partnerships Across agencies, institutions and the community

32 What are your thoughts? Any questions on the program design, implementation or evaluation? Do you know of a similar program in your area? Are there opportunities for such a program in your community?

33 Acknowledgement Appalachian Farmacy Committee and partners during the launch at the Johnson City s Farmers Market in downtown Johnson City.
34 For More Information K. Munene Mwirigi