Future treatment of hemophilia: Spoiled for choice
|
|
|
- Hugo Shepherd
- 5 years ago
- Views:
Transcription

1 Future treatment of hemophilia: Spoiled for choice David Lillicrap Department of Pathology and Molecular Medicine Queen s University Kingston, Canada Bangkok, November 2017
2 Disclosures for David Lillicrap In compliance with COI policy, ISTH requires the following disclosures to the session audience: Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Bayer, Bioverativ, CSL, Octapharma No relevant conflicts of interest to declare No relevant conflicts of interest to declare No relevant conflicts of interest to declare No relevant conflicts of interest to declare No relevant conflicts of interest to declare No relevant conflicts of interest to declare Presentation includes discussion of the following off-label use of a drug or medical device: <N/A>
3 Hemophilia Therapy Replace the missing/defective protein Clotting Factor Source A. Donated Plasma - History of infectious risk B. Recombinant DNA Production Genetically Engineered 1. Chinese Hamster Ovary Cells 2. Baby Hamster Kidney Cells 3. HEK293 Cells
4 Hemophilia Treatment Limitations Requires frequent intravenous injections - (Q1-3 days) ~30% incidence of anti-fviii antibodies in hemophilia A Expensive (annual Canadian clotting factor budget ~$230 million) Limited global access to treatment. (~30% of patients have access)
5 Innovative Strategies for Hemophilia Therapy Extended half-life products. (Half-lives FVIII 12hrs/FIX 24hrs) Intrinsic tenase innovations Inhibitors of anticoagulant mechanisms Gene therapy
6 Novel Clotting Factor Concentrates 1. Modified native protein - Single chain covalently linked FVIII (CSL) 2. Molecular conjugates - PEGylation (Baxter, Novo Nordisk, Bayer) - XTENylation (Biogen) - PASylation (Generium) 3. Fusion proteins - IgG (Biogen) - Albumin (CSL)
7 Clotting Factor Half-Life Extensions Factor IX 3 to 5-fold (Santagostino et al Blood 2012) (Negrier et al Blood 2011) (Shapiro et al Blood 2012) 1 infusion Q7-14 days Factor VIII 1.5 to 1.8-fold 1 infusion Q3-4 days (Powell et al Blood 2012) (Coyle et al JTH 2014) (Mahlangu et al Blood 2014) FVIII half-life limited by dominance of VWF
8 Novel, Non-factor Replacement Therapy for Hemophilia Generation of a Novel Intrinsic Tenase Complex Factor VIII mimetic
9 Intrinsic Tenase Complex FIXa FX FXa FVIIIa Ca 2+ Ca 2+ Activated Phospholipid Surface Platelet Endothelium WBC
10 Intrinsic Tenase Complex in Hemophilia A FIXa FX FXa 200,000-fold Reduced Catalytic efficiency Ca 2+ Ca 2+
11 ACE910 bispecific antibody: (Emicizumab) FIXa FX FVIII mimetic bispecific Ab ACE910 Ca 2+ Ca 2+ Chugai Genentech Roche
12 Effect of Bispecific Antibody on Intrinsic Tenase Catalytic Efficiency FIXa alone 1 k cat /K m + Bispecific Ab 19,800 + FVIIIa 272,000 Kitazawa T et al. Nat Med 2012;18:
13
14 FVIII Mimetic Bispecific Antibody (Emicizumab: Chugai Genentech Roche) 109 hemophilia A pts with FVIII inhibitors enrolled Weekly subcutaneous Emicizumab 87% reduction in annualized bleeding rate with Emicizumab 63% of pts on Emicizumab prophylaxis had zero bleeds
15 Reduction of Annualized Bleeding with Weekly Prophylactic Emicizumab
16 Wednesday Nov 2 nd 2016 Roche Public Announcement 4 FVIII inhibitor patients have experienced SAEs Being treated for breakthrough bleeds with ACE910 and repeated high dose FEIBA 2 pts - venous thromboembolic events 2 pts - thrombotic microangiopathy
17 Emicizumab Phase 3 Clinical Trials Haven 1 - Adult FVIII Inhibitor pts (109 pts) - Completed ISTH Berlin/NEJM Haven 2 - Pediatric FVIII Inhibitor pts Haven 3 - Adult Non-inhibitor pts **** Haven 4 - Monthly dosing schedule **** Potential for major disruptive technology
18 Balanced Hemostasis FVIII FIX FXI FX FVII FII Fibrinogen AT PS PC TFPI
19 Unbalanced Hemostasis Hemophilia A FVIII FIX FXI FX FVII FII Fibrinogen Bleeding AT PS PC TFPI
20 Unbalanced Hemostasis - Antithrombin Deficiency FVIII FIX FXI FX FVII FII Fibrinogen AT PS PC TFPI Thrombosis
21 Re-Balanced Hemostasis FVIII FIX FXI FX FVII FII Fibrinogen Fitusiran - Antithrombin sirna AT PS PC TFPI Ragni M. NEJM 2015; 373
22 Re-Balanced Hemostasis FVIII FIX FXI FX FVII FII Fibrinogen Concizumab Anti-TFPI Ab Bayer Pfizer Anti TFPI Abs AT PS PC TFPI Ragni M. NEJM 2015; 373
23 Re-Balanced Hemostasis FVIII FIX FXI FX FVII FII Fibrinogen AT PS PC - TFPI APC Ragni M. NEJM 2015; 373
24 Rebalancing Hemostasis Strategies In principle, have the potential to work in all procoagulant deficient states a) Including patients with some rare bleeding disorders b) Including patients with inhibitors
25 Reducing its production - sirna Inhibiting Antithrombin Inhibiting its function - Antibody/Aptamer/Peptide Anti-TFPI antibodies Inhibiting TFPI Inhibiting Activated Protein C Novel bioengineered Anti-APC Serpin

26
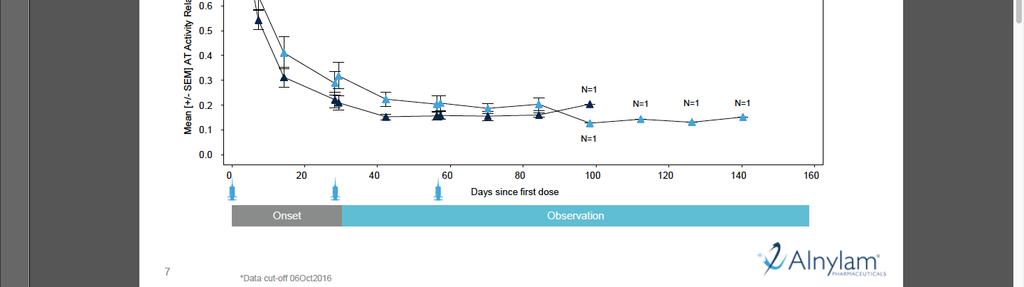
27 Fitusiran ASGPR (ph>5) Clathrin-coated pit AT Recycling ASGPR Clathrin-coated vesicle Fitusiran (anti-at3 sirna) RISC Endosome mrna Nucleus 27 Fitusiran (ALN-AT3) SC-administered small interfering RNA (sirna) therapeutic targeting antithrombin (AT)
28 Inhibiting Antithrombin Delivery and duration of action Subcutaneous injection Weekly - monthly Sehgal A et al. Nat Med 2015;21:492 7.

29 Slide No. 29

30 Peak Thrombin Levels Achieved in Hemophilia A and B Patients Treated with Fitusiran
31 Annualized Bleed Rates in Hemophilia Patients with Inhibitors Treated with Fitusiran Follow up days
32 Alnylam Pharmaceuticals News Release Sept 7 th 2017 Alnylam is reporting a fatal thrombotic event in a patient with hemophilia A without inhibitors in the Phase 2 open-label extension (OLE) study of fitusiran...investigation of the SAE, including review of the patient's CT scans by three independent neuro-radiologists, who all confirmed on September 1, 2017, that the initiating event was a cerebral venous sinus thrombosis.

33 Hemophilia gene therapy: great expectations 23 rd March 1994


34 Gene Therapy: Therapeutic Effects in Clinical Trials Leber's congenital amaurosis Ali RR, Bennett J Cancer Rosenberg SA, Morgan RA. June C SCID-X1 SCID-ADA Thalassemia Wiskott-Aldrich syndrome Cavazzano-Calvo M, Fischer A, Hacein-Bey-Abina S. Aiuti A, Bordignon C, Roncarolo MG. Thrasher A. Leboulch P. Klein C Adrenoleukodystrophy Metachromatic leukodystrophy Cartier N, Aubourg P. Naldini L, Biffi A Epidermolysis bullosa Mavilio F Haemophilia Nathwani AC, Davidoff AM Graft-versus-host disease Bonini C. 2012
35 Strategies for transgene delivery (1) Direct in vivo gene transfer PRO s: Practically easy Minimal time commitment CON s: In vivo exposure of vector: immune response Variable vector targeting efficiency 35
36 Strategies for transgene delivery (2) Indirect ex vivo gene transfer Harvest/isolate autologous, long-lived progenitor cells Deliver normal clotting factor gene PRO s: No in vivo vector exposure Direct cell targeting CON s: Very labor intensive Requires host conditioning Expand cell numbers 36
 PRO s Wild type AAV minimally pathogenic in humans Many different serotypes (capsid proteins) CON s Small packaging capacity (~5")
37 Transgene Delivery Vehicles 1. Adenovirus: pro inflammatory Lentivirus: production challenges 3. Adeno associated virus (AAV) PRO s Wild type AAV minimally pathogenic in humans Many different serotypes (capsid proteins) CON s Small packaging capacity (~5 kb) Pre existing immunity in humans: 30 60% AAV 22 nm 37
38 Wild type AAV: 4.7 kb Single Stranded DNA Genome ITR Rep Cap ITR Enhancer- Promoter Transgene cdna ITR AAV transgene construct ITR 38 FIX cdna 1.3 kb B domain-deleted (BDD) FVIII cdna ~4.7 kb
39 Hemophilia gene therapy: initial proof of sustained benefit Adenovirus-Associated Virus Vector Mediated Gene Transfer in Hemophilia B Amit C. Nathwani, M.B., Ch.B., Ph.D., Edward G.D. Tuddenham, M.B., B.S., M.D., Savita Rangarajan, M.B., B.S., Cecilia Rosales, Ph.D., Jenny McIntosh, Ph.D., David C. Linch, M.B., B.Chir., Pratima Chowdary, M.B., B.S., Anne Riddell, B.Sc., Arnulfo Jaquilmac Pie, B.S.N., Chris Harrington, B.S.N., James O Beirne, M.B., B.S., M.D., Keith Smith, M.Sc., John Pasi, M.D., Bertil Glader, M.D., Ph.D., Pradip Rustagi, M.D., Catherine Y.C. Ng, M.S., Mark A. Kay, M.D., Ph.D., Junfang Zhou, M.D., Yunyu Spence, Ph.D., Christopher L. Morton, B.S., James Allay, Ph.D., John Coleman, M.S., Susan Sleep, Ph.D., John M. Cunningham, M.D., Deokumar Srivastava, Ph.D., Etiena Basner-Tschakarjan, M.D., Federico Mingozzi, Ph.D., Katherine A. High, M.D., John T. Gray, Ph.D., Ulrike M. Reiss, M.D., Arthur W. Nienhuis, M.D., and Andrew M. Davidoff, M.D 39 Nathwani AC, et al. N Engl J Med 2011;365:
40 Hemophilia Gene Therapy initial proof of sustained benefit Subject 8: dosed 2x10 12 vg/kg - AAV8 FIX gene delivery (peripheral vein) FIX hfix:c (IU/dL) hfix ALT ALT (IU/l) Weeks post vector infusion 40 Nathwani AC, et al. N Engl J Med 2011;365:
41 Hemophilia Gene Therapy Clinical Trials: 2017 Factor IX 1. UCL/St Jude AAV8 codon optimized FIX 2. Spark Therapeutics novel AAV FIX Padua 3. UniQure AAV5 codon optimized FIX 4. Baxalta/Shire AAV8 FIX Padua 5. Dimension Therapeutics AAV10 FIX 6. Sangamo AAV6 FIX safe harbour
42 Factor IX Padua: Gain-of-function FIX Mutant 7-fold increase Use in FIX gene therapy Simioni P et al. New Engl J Med 2009; 361:
43 Results with SPK-9001 Factor IX Gene Therapy Trial 5 x vg/kg (no prophylactic steroids)

44 Spark 9001 Clinical Outcome Data Bleeding Rates Pre and Post Gene Transfer Pre: Post: FIX Protein Infusions Pre and Post Gene Transfer Pre: Post:
45 Hemophilia Gene Therapy Clinical Trials: 2017 Factor VIII 1. Biomarin AAV5 codon optimized FVIII 2. UCL AAV8 codon optimized FVIII/V3 B domain 3. Spark Therapeutics AAV SPK Sangamo AAV2/6 SB-525 BDD FVIII

46 July 10 th 2017
47 Biomarin BMN 270 AAV5 FVIII Study 15 Subjects - 4 Dose Cohorts 1 subject - 6 x 10e12 1 subject - 2 x 10e13 6 subjects - 4 x 10e13 7 subjects - 6 x 10e13

48

49 BMN 270 Annualized Bleed Rates

50 Is AAV-Mediated Liver Gene Transfer Curative for Hemophilia? Severe hemophilia A & B dogs follow up 10+ years Severe hemophilia B patients Follow up for 7+ years Large animal & human results show long-term factor expression following single infusions of AAV vectors to the liver
51 Hemophilia Gene Therapy Challenges: September 2017 Pre-existing anti-aav immunity - (~50%) Transient AAV-associated liver toxicity Questions of long-term genotoxicity Capacity for vector production
52 Hemophilia Gene Therapy Complications 1. Hepatotoxicity 4 12 week onset Response to steroids AAV-capsid specific CD8 T cells sometimes detectable Pathogenetic mechanism remains debatable
53 Hemophilia Gene Therapy Complications 1. Hepatotoxicity 4 12 week onset Response to steroids AAV-capsid specific CD8 T cells sometimes detectable Pathogenetic mechanism remains debatable 2. Long-term genotoxicity? Potential risk of hepatocarcinoma??? Sites of AAV integration are random and appear non-oncogenic

54 Global Hemophilia Market Value 8.5 billion 5.6% annual growth Market Research Report August 2016
55 Conclusions 1. The treatment for hemophilia over the past 2 decades, involving protein replacement, has been safe and effective.
56 Conclusions 1. The treatment for hemophilia over the past 2 decades, involving protein replacement, has been safe and effective. 2. Over the past 5 years, there have been dramatic advances in hemophilia treatment innovation.
57 Conclusions 1. The treatment for hemophilia over the past 2 decades, involving protein replacement, has been safe and effective. 2. Over the past 5 years, there have been dramatic advances in hemophilia treatment innovation. 3. A range of new hemophilia therapies is now entering the clinic that will require careful consideration to match treatment choices with individual patients. Serious adverse events have been documented with several of these therapies.
58 Conclusions 1. The treatment for hemophilia over the past 2 decades, involving protein replacement, has been safe and effective. 2. Over the past 5 years, there have been dramatic advances in hemophilia treatment innovation. 3. A range of new hemophilia therapies is now entering the clinic that will require careful consideration to match treatment choices with individual patients. Serious adverse events have been documented with several of these therapies. 2. The economics of these treatment advances remains to be resolved.

59 View from Richardson Laboratory Queen s University, Kingston, Canada