Peripheral Venous Catheter and Central venous catheter care : an IVN Approach. Nutcharee Jungvanichar RN, MBA
|
|
|
- Jeremy Alexander
- 5 years ago
- Views:
Transcription
1 Peripheral Venous Catheter and Central venous catheter care : an IVN Approach Nutcharee Jungvanichar RN, MBA
2 Anatomy of vein Purpose of IV Therapy Skin preparation IV Starting IV Catheter and IV Device Flushing protocol Site care maintenance Documentation Central line care Agenda

3 From Practice with International Standard

4 Anatomy of Vein
5 Veins of the Upper Extremities Digital Vessels -Along lateral aspects fingers, infiltrate easily, painful, difficult to immobilize and should be your LAST RESORT Metacarpal Vessels -Located between joints and metacarpal bones (act as natural splint) -Formed by union of digital veins -Geriatric patients often lack enough connective / adipose tissue and skin turgor to use this area successfully Digital
6 Veins of the Upper Extremities Cephalic (Intern s Vein) -Starts at radial aspect of wrist -Access anywhere along entire length (BEWARE of radial artery/nerve) Medial Cephalic ( On ramp to Cephalic Vein) -Joins the Cephalic below the elbow bend -Accepts larger gauge catheters, but may be a difficult angle to hit and maintain

7 Veins of the Upper Extremities Basilic - Originates from the ulner side of the metacarpal veins and runs along the medial aspect of the arm. It is often overlooked becauses of its location on the back of the arm, but flexing the elbow/bending the arm brings this vein into view Medial Basilic - Empties into the Basilic vein running parallel to tendons, so it is not always well defined. Accepts larger gauge catheters. - BEWARE of Brachial Artery/Nerve



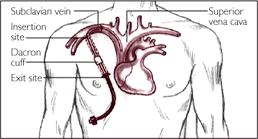

8 Central Venous Catheter Sites PICC (Peripherally inserted Central Catheter) Percutaneous(Subclavian) Implanted Port (single or double lumen) Tunnelled (Hickman) Percutaneous (IJ-Int. Jugular)
9 Purposes of IV Therapy To provide parenteral nutrition To provide avenue for dialysis/apheresis To transfuse blood products To provide avenue for hemodynamic monitoring To provide avenue for diagnostic testing To administer fluids and medications with the ability to rapidly/accurately change blood concentration levels by either continuous, intermittent or IV push method.
10 Infusion Equipment Flow - control device Electronic infusion device with administration based, anti free flow mechanisms shall be used Dose error reduction system shall be considered in selection and use of electronic infusion devices The nurse should be involved in the evaluation and selection of flow control devices

11 Infusion Equipment Tourniquets The tourniquet should be single-patient use Latex allergy should be assesses


12 Closed Infusion System Closed Infusion Container- Fully collapsible plastic container without air filter
13 Skin preparation Wash your hand Put on Glove Clean the site Use antiseptic Scrub with friction Allow the antiseptic agent to dry thoroughly(15 Sec.)

14 Which one is preferred
15 Starting a Peripheral IV Finding a vein can be challenging Go by feel, not by sight. Good veins are bouncy to the touch, but are not always visible. Use warm compresses and allow the arm to hang dependently to fill veins. A BP cuff inflated to 10mmHg below the known systolic pressure creates the perfect tourniquet. Arterial flow continues with maximum venous constriction. Using a tourniquet may provide better venous congestion Avoid areas of joint flexion Start distally and use the shortest length/smallest gauge access device that will properly administer the prescribed therapy

16 How many attempt we can do???

17 : CPG

18 PIV Catheter 3 kind of IV catheter PVC Tavlon Polyurethane ETFE catheter tetrafluoroethelene Polyurethane : decrease phlebitis rate up to 40%


19 IV Cap Add on device(ins) The use of stopcock is not recommend to use due to the increased risk of infection

20 Microbial contamination Contamination of Stopcock Entry Ports on Central Venous Catheters Tebbs et al, Intensive Care Med.1996;22:


21 Needless Connector Needless connector are changed if there is blood or debris visible within the needless connector, upon contamination, prior to drawing a blood culture through a catheter, and routine as established by the organization


22 IV dressing Gauze and Tape Transparent dressing


23 Flushing Protocol NSS flush > Flush more Heparin Flush
24 Slow clamp method Push and pause method Flushing Method
25 Flush the device Clean the port : scrub 15 second Slow inject, maintain positive pressure For needless connector : should neutral pressure device
26 Site care and maintenance Primary and continuous administration set should be change no more than 96 hrs. ( INS 2011) If secondary administration set is detached from the primary set>>> consider as an intermittent IV set Intermittent IV set should be changed every 24 hrs. (INS2011, CDC..) IV Set for TPN, Lipid >>> 24 hrs. Blood set >>> 4 hrs.
27 Filters Filters are use to prevent the passage of undesirable substance into the vascular The specific type an size of filter used is determined by the infusate and may be an add on device or an integral part of administration set A 0.2 micron filter that is bacteria and particulate-retentive and air eliminating is used with non lipid-containing solution that require filtration A0.2 micron filter that is surfactant free, particulate-retentive, and air-eliminating is used with intraspinal infusions A 1.2 micron that is particulate-retentive and air eliminating is used with lipid infusion or 3 in 1 parenteral infusion Small volume infusion of 5 ml or less over 24 hours and IV push medication should not be administered through a 0.2 micron filter INS 2011
28 Types of IV Fluid Containers There are generally three types of IV fluid containers in use globally. Rigid containers which are made of glass, High Density Polyethylene (HDPE) or Polypropylene (PP) Semi-rigid containers which are made of Polyethylene (PE) or Polypropylene (PP) Flexible bags which are made of polyvinyl chloride (PVC), or Polyolefin laminate


29 Open Infusion Container Glass container with air filter. Open Infusion Container Semi-rigid container with air filter. Open Infusion System
30 Open Infusion System The chance of contamination in an open system is 10 times more than the closed system. Any device which has tubes with one end inside the body and one outside can cause contamination. These include urinary catheters, IV fluid bags, endotracheal tube, etc. These should be closed systems so as to prevent contamination.
31 Documentation Able to identify the person providing care : เข ยนอ านออก บอกได ว าใคร Document must be completed with Specific site preparation Device: Length and gauze Date and time of insertion Insertion site Dressing type Type of therapy Patient/ relative s understanding, education Upon removal: condition of site, patient response, patient education When multiple access device or catheter lumens are use, documentation should clearly indicate what fluid/medication are being through each pathway.
32 Documentation IV puncture Date and time Number of IV catheter Location of insertion site: anatomical name if possible Number attempt of venipuncture Patient teaching and evidence of patient understanding Initial name
33 Example of IV documentation Date and time January 3,2015 January 6,2015 Intervention IV catheter No 22 was inserted at left metacarpal vein with first attempt. Transparent dressing was applied, insertion site was clean, dry, intact. Patient instruction was given and patient state I will call a nurse if the problem is occurred. Nutcharee J. RN IV catheter was removed from left metacarpal vein. Skin is dry clean and intact. Patient state it doesn t hurt. Patient education are provide. Nutcharee J
34 IV removal protocol Wash your hand Put on glove Remove dressing with aseptic technique Remove IV catheter with pressure Cover IV removal site with sterile dressing Re-evaluate IV site 24 hrs. after removal
35 Central line Bundle Hand Hygiene Maximal Barrier Precautions Chlorhexidine Skin Antisepsis Optimal Catheter Site Selection Assessment of Central Line Necessity
36 CLABSI CLABSI is the term used by the US Centers for Disease Control and Prevention s (CDC s) National Healthcare Safety Network (NHSN) 9 (see NHSN CLABSI information). A CLABSI is a primary bloodstream infection (that is, there is no apparent infection at another site) that develops in a patient with a central line in place within the 48-hour period before onset of the bloodstream infection that is not related to infection at another site. Culturing the catheter tip or peripheral blood is not a criterion for CLABSI. CRBSI is a more rigorous diagnostic definition and requires specific laboratory testing to identify the catheter as the source of the bloodstream infection, such as culturing the catheter tip or a more elaborate method such as differential time-to-positivity of blood cultures. The Joint commission tool kits
37 CLABSI Prevention Strategies, Techniques, and Technologies Basic education, and particularly education with feedback of CLABSI rates to staff, can result in lower CLABSI rates Hand hygiene is a key component Aseptic technique maximal sterile barrier precautions, skin preparation, catheter selection, and use of catheter kits or carts Using an insertion checklist
38 CLABSI Prevention Strategies, Techniques, and Technologies The insertion process must be focused catheter site selection insertion under ultrasound guidance catheter site dressing regimens securement devices Insertion bundle Proper maintenance of CVCs Scrub the hub, connectors, and injection ports Dressing changing protocol daily review of line necessity

39 Bundle Kits/Line Cart


40 Catheter Securement Device
41 INS update 2016 Catheter stabilization is recognized as an intervention to decrease the risk of phlebitis, catheter migration and dislodgement, and may be advantage in preventing CRABSIs. Pathogenesis of CRBSIs occurs via migration of skin flora through the percutaneous entry site. Sutureless securement devices avoid disruption around the catheter entry site and may decrease the degree of bacterial colonization.

42 Phlebitis rate Infiltration rate Extravasation CLABSI Process& outcome Skin preparation Site selection Proper equipment Dressing Site cleaning Port cleaning preparation Flushing protocol Maintenance management Monitoring Harvest (outcome)
43 Conclusion Preparation Insertion Maintenance removal Do the right thing right at the first time