DISSERTATION ON STUDY ON THE PREVALENCE OF BETA LACTAMASES IN GRAM NEGATIVE CLINICAL ISOLATES
|
|
|
- Norman Norris
- 5 years ago
- Views:
Transcription



1 DISSERTATION ON STUDY ON THE PREVALENCE OF BETA LACTAMASES IN GRAM NEGATIVE CLINICAL ISOLATES Dissertation submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY in partial fulfilment of the requirement for the award of degree of MD BRANCH IV MICROBIOLOGY KARPAGA VINAYAGA INSTITUTE OF MEDICAL SCIENCES, MADURANTAGAM. THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY, CHENNAI, TAMILNADU. APRIL 2016



2 DISSERTATION ON STUDY ON THE PREVALENCE OF BETA LACTAMASES IN GRAM NEGATIVE CLINICAL ISOLATES Dissertation submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY in partial fulfilment of the requirement for the award of degree of MD BRANCH IV MICROBIOLOGY KARPAGA VINAYAGA INSTITUTE OF MEDICAL SCIENCES, MADURANTAGAM THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY,. CHENNAI TAMILNADU. APRIL 2016
3 CERTIFICATE Certified that this dissertation entitled STUDY ON THE PREVALENCE OF BETA LACTAMASES IN GRAM NEGATIVE CLINICAL ISOLATES is a bona fide work done by Dr. S.Sarasa, Post graduate student, Karpaga Vinayaga Institute of Medical Sciences, Madurantagam, during the academic year Dr.A.R. Chakravarthy MD DGO, Dean, Karpaga Vinayaga Institute of Medical Sciences and Research Centre Madurantagam Taluk, Kancheepuram Dist Tamil Nadu, India. Dr T.S.Vijayalakshmi M.D Professor &Head Dept. of Microbiology, Karpaga Vinayaga Institute of Medical Sciences and Research Centre Madurantagam Taluk, Kancheepuram Dist , Tamil Nadu, India.
4 DECLARATION I declare that the dissertation entitled Study on the prevalence of beta lactamases in gram negative clinical isolates submitted by me for the Degree of M.D is the record work carried out by me during the period of April 2014 to March 2015 under the guidance of Dr.T.S Vijayalakshmi M.D. PROFESSOR and H.O.D of Microbiology, Karpaga Vinayaga Institute of Medical Sciences and Research Centre and has not formed the basis of any Degree,Diploma, Fellowship titles in this or any other University or other similar Institution of Higher learning. Signature of the candidate Place: Dr.S.Sarasa Date: Signature of the guide Dr T. S. Vijayalakshmi Professor & H.O.D Karpaga Vinayaga Institute of Medical Sciences and Research Centre, Madurantagam.
5 ACKNOWLEDGEMENT I express my sincere thanks to Dr. R. Annamalai, Managing Director, Karpaga Vinayaga Institute of Medical Sciences for his kindness in helping with all available resources. I wish to thank Dr. A.R. Chakravarthy, Dean Karpaga Vinayaga Institute of Medical Sciences for his valuable support and encouragement. It is beyond words to express my sincere thanks and gratitude to my teacher and guide Dr. T.S. Vijayalakshmi, Professor and Head of Department of Microbiology, KIMS who consistently guided me in each and every step of my thesis work. Her kind support and encouraging words are great pillars of my success. I wish to proudly thank my teacher and professor Dr. D.Joseph Pushpa Innocent and Dr. T.Sheila Doris for their valuable advice and support. It also gives immense pleasure in thanking Assistant professors, Dr. K.Balan Dr. A.V.Sangeetha, Dr. J.Abirami Lakshmy and tutor Mrs. E.Vanitha Devi, for helping me in overcoming difficult situations during this thesis work and for their valuable guidance. I also thank my technical staff Mr Devaraj, Mrs.Amudha, Miss Puspha and Miss Punitha and nontechnical staff of Department of Microbiology for their excellent help in laboratory work.
6 My completion of thesis would have not been accomplished without the support of my family who are always a pillar of strength in all my endeavours. Above all I thank the Almighty for His blessings.

























7
8 TABLE OF CONTENTS S. NO. TITLE PAGE NO. 1. INTRODUCTION 1 2. AIMS AND OBJECTIVES 5 3. REVIEW OF LITERATURE 6 4. MATERIALS AND METHODS RESULTS DISCUSSION SUMMARY CONCLUSION ANNEXURES 10. BIBLIOGRAPHY
9 Introduction
10 1. INTRODUCTION Antimicrobial resistance is really a threat to clinical practice. Bacteria develop various mechanisms of resistance to different group of antibiotics. Antimicrobial resistance is the resistance of a microorganism to an antimicrobial drug that was originally effective for treatments of infections caused by it, by acquiring genes coding for it. Antimicrobial resistance is a global concern, as new resistance mechanism evolve, making the treatment of even common infections difficult resulting in disability or death of individual. β lactamases production is one of the most important mechanisms of microbial resistance to β-lactam antibiotics which consist of four major groups such as,penicillins, Cephalosporins, Monobactams, and Carbapenems. Excessive use of antibiotic results in selective pressure, enabling resistant bacteria to thrive, and the beta lactamase gene undergoes continuous mutation. (1) Certain acquired mechanism such as plasmids help in exchange of resistant determinants which has become a threat to clinicians as these cause rapid dissemination of genes between species. The enzymes produced by bacteria are usually distinguished into four types, out of which 3 form major group,such as extended spectrum β- lactamases (ESBL), class C Cephalosporinases (AmpC)) and β-lactamases with 1
11 carbapenemase activity in which metallo -β-lactamases (MBL)is of great concern today. (2) In the early 1980s, the third-generation Cephalosporins which were very effective were introduced for treating beta lactamase mediated resistance. The advantages of these drugs were decreased nephrotoxic effects when compared to Aminoglycosides and Polymyxin. (3) E.coli and Klebsiella are leading causes of pneumonia, UTI, diarrhea, cholecystitis, meningitis. β lactam antibiotics has been the drug of choice in treating these conditions. However multiple antibacterial resistances in recent decades among Enterobacteriaceae are commonly met and the above conditions and pose a problem in management. (4) Over the past few years the occurrence of multidrug-resistant Gramnegative bacteria has increased due to multiple mechanism of resistance, which is a continuous phenomenon. The major concern is the production of AmpC beta-lactamases and/or extended-spectrum beta-lactamase in bacterial strains. ESBL s confer resistance to, Cephalosporins, Oxyimino-cephalosporins (e.g., Ceftriaxone, Cefotaxime, and ceftazidime) Amino- penicillins and AmpC betalactamases in addition are resistant to Cephamycin (e.g., Cefoxitin) and Monobactams. (5) 2
12 ESBLs are still a threat to clinicians as they are coded by plasmid and can be easily transmitted between species. ESBL producing organisms are highly effective in inactivating Pencillins, most Cephalosporins and Aztreonam Amp C beta lactamases are of either chromosomal, or plasmid mediated. The transfer of chromosomal genes onto plasmids results in lactamases called as inducible Amp c lactamases. Hence Amp C β isolates of Enterobacter aerogenes, Salmonella, Escherichia coli, Klebsiella, and Citrobacter have acquired plasmid mediated Amp C beta lactamases. (6) Various risk factors are involved for the infection or colonization with the ESBL producing organisms. Prolonged stay in the hospital or ICU, Persons with vascular or urinary catheters, and those undergoing haemo- dialysis or emergency abdominal surgery also fall in this group. The prior antibiotic therapy to any antibiotic such as Aminoglycoside, Quinolones, Trimethoprim- Sulfamethoxazole, and Metronidazole or gut colonization with resistant bacteria also predisposes to acquisition of a resistant microbe. (7) With the introduction of Carbapenem, there came an end to war against antimicrobial resistance till Carbapenamase enzymes emerged. These were useful drugs as they had broad spectrum of activity to combat infection caused by Pencillin and Cephalosporin resistant bacteria. (8) Resistance to Carbapenem is predominantly mediated by metallo-beta lactamases, a class B type of beta lactamases that require bivalent metal ions 3
13 for activation. Hence detection of these β lactamases producing organisms becomes important for effective therapeutic approach and enhanced infection control. This study aims at detecting the prevalence of ESBL, Amp C and carbapenamases production in our hospital. 4
14 Aims and Objectives
15 2. AIMS & OBJECTIVES 2.1 To know the antimicrobial susceptibility profile of the gram negative bacilli included in the study. 2.2 To study the prevalence of resistance in gram negative clinical isolates. 2.3 to determine the resistance pattern among the gram negative isolates. 2.4 To find the prevalence of ESBL, Amp C Carbapenamases production and their combinations {ESBL +Amp C; ESBL +MBL; Amp C +MBL} in the isolates. 5
16 Review of Literature
17 3. REVIEW OF LITERATURE Antibiotics discovery has revolutionized medicine in the 20 th century, as wonder drugs, but regrettably, the concomitant rise of antibiotic resistance in hospitals, communities, and the environment have evolved with their use. Man's misuse and overuse of antibiotics accelerates the microbes to develop resistance genes, and horizontal gene transmission occurs. Hence for every antibiotic discovered organism tend to develop multiple mechanisms of resistance. (9) 3.1. ANTIBIOTIC HISTORY Antibiotics are special kind of chemotherapeutic agent obtained from living organism. The antibiotic era began70 years ago with the development of Pencillin. Some observations suggest that even before the extensive use of penicillin, bacteria had mechanism to destroy Pencillin by enzymatic degradation. It was a finding by Abraham and Chain, 1940). (10) The word ANTIBIOTIC refers to a metabolic product of one organism that in small amounts kills or inhibits another microorganism [12] Word antibiotic was coined by Washman in 1945 (10). In earlier days Europeans used natural quinine from bark of cinchona to treat malaria. Mercury was used to treat syphilis, until arsenical compound salvarasan known as magic bullet was identified by Paul Erhlich. In 1914 he announced the discovery of neosalvarasan and henceforth he is known as Father of 6
18 Chemotherapy. Syphilis was the first known disease for which chemotherapeutic agent was used. (12) In 1928 Alexander Fleming made accidental discovery of penicillin from the fungus Pencillium notatum, which produces a substance that destroys Staphylococci, this substance was later named penicillin (13). The advent of modern antibiotic era was developed only after Gerhard Domagh found that prontosil [forerunner of Sulphonamides] had dramatic effect on Streptococcal infections in He exploited the potential for antibiotic production among soil organisms (12). In 1940, it was found that Pencillin could be effective therapeutic substance. The discovery of antimicrobials, laid a path for research on chemotherapeutic agents and future drug discovery. This resulted in a number of new antibiotics, some of which made their way for clinical use. (10)(16) The next two decades was indeed the golden era, during which the discovery of novel antibiotics occurred, with no new classes further discovered (10). The golden age of antibiotics will soon come to an end, if the evolution of antibiotic resistance is not hampered, or if replacements for them are not found ANTIBIOTIC RESISTANCE It is the ability of microorganism to grow in the presence of a chemical (drug) that normally kills or limits its growth. Resistant strains which are capable of inactivating the drug became prevalent, as the antibiotic was widely used and 7
19 studies were undertaken to modify penicillin molecule so as to prevent the action by Pencillanases. (9) 3.3 SUPERRBUGS AND SUPER RESISTANCE Microbes with enhanced morbidity and mortality acquired due to multiple mutations are termed as superbugs. These endow high levels of resistance to the antibiotic classes which are specifically recommended for their treatment. Thus the choice of treatment for these microbes are decreased and making it more costly. Even the periods of hospital care is extended. Super resistant strains have acquired increased virulence, and enhanced transmissibility in some cases. In reality, antibiotic resistance can be considered a virulence factor for the organism. (9) A strong correlation between antibiotic use and development of antibiotic resistance in the treatment of the diseases caused by Gram-negative pathogens, such as Escherichia coli, Salmonella enterica, and Klebsiella pneumoniae, has been observed in the past half-century. These organisms cause variety of infections in humans and animals. This is especially observed with the β-lactam class of antibiotics and the β-lactamases which are their related inactivating enzymes,. 3.4CLASSIFICATION OF ANTIBIOTICS Antibiotics are classified on basis of method of action on bacteria. They act by inhibiting the synthesis of cell wall, damaging the cytoplasmic membrane. The other mechanisms are inhibition of nucleic acid or protein 8
20 synthesis and inhibition of specific enzyme pathway. (14) β lactam antibiotics fall under the group of cell wall inhibitors. 3.5 CELL WALL SYNTHESIS INHIBITORS bacteria. These are agents which exert their effect by acting on the cell wall of 3.5.1βlactam antibiotics Pencillin, Cephalosporins, Methicillin, Carbapenem, Monobactams, come under this group. They are broad class of antibiotics characterized by a beta lactam ring which is as the core structure and the key to the mode of action of this class of antibiotics. β- Lactam antibiotics act by inhibiting cell wall synthesis of bacteria. The beta lactam ring binds to PBPs, preventing the cross linking of cell walls. They target the pencillin binding protein (PBP) {transpeptidases}, which are involved in, rendering them unable to perform their role in cell wall synthesis. (15) Mechanism of Action of β-lactam antibiotics: Bacteria synthesize UDP N Acetyl muramic acid pentapeptide and UDP N Acetyl glucosamine pentapeptide residues, which are linked together. UDP is split of leading to final step of cleavage of the terminal D- alanine of the peptide chains by transpeptidases and cross linking between peptide chains of the neighboring strands occurs, β-lactam antibiotic inhibits 9
21 transpeptidases so that cross linking is not formed and thereby inhibiting the replication of bacteria. Mechanism of action of beta lactam antibiotics is by inhibition of cell wall synthesis. The antibiotic gets incorporate into the bacterial cell wall and inhibit transpeptidases, which help in cell wall synthesis. Secondly, they attach to the Penicillin binding proteins and lyse the bacterial cell wall by freeing the cell wall hydrolases. Bacteria resist these antimicrobial mechanisms of action, by producing β lactamases or mutated types of penicillin binding proteins. (18) 3.6. β LACTAM ANTIMICROBIAL AGENTS The β lactam antibiotics are classified as follows, (17) 1. Penicillins: Penicillin G, Penicillin 2. Penicillinase resistant Penicillins: Methicillin, Nafcillin, Oxacillin, and Cloxacillin 3. Ureidopenicillins: Mezlocillin, Piperacillin 4. Aminopenicillins: Ampicillin, Amoxicillin 5. Carboxy penicillins: Carbenicillin, Ticarcillin 6. Cephalosporins : a. First generation: Cefazolin, Cephalothin, Cephalexin b. Second generation: Cefuroxime, Cefaclor, Cefamandole, Cefamycins (Cefotetan, Cefoxitin) c. Third generation: Cefotaxime, Ceftriaxone, Cefpodoxime, Ceftizoxime, Cefoperazone, Ceftazidime 10
22 d. Fourth generation: Cefepime, Cefpirome 7. Carbapenems: Imipenem, Meropenem, ertapenem 8. Monobactams: Aztreonam. STRUCTURE OF BETA LACTAM ANTIBIOTICS 1. PENCILLINS: Pencillins are group of natural or semi synthetic compounds containing chemical nucleus 6 aminopencillanic acids which has β lactam ring fused to thiazolidine ring. The other rings vary in respect of each group of antibiotics. Pencillins differ from one another by substitution position 6. (2 1) 11







23 2. CEPHALOSPORINS Cephalosporins are fermentation products of Cephalosporium acremonium. They contain 7 cephalosporanic acids which has β lactam ring fused to dihydrothiazine ring. They are classified to four generations according to their profile of action. 3. MONOBACTAMS These are compounds in which the beta lactam ring is alone and not fused..aztreonam was isolated from Chromobacterium violaceum. It is unique 12
24 in being active only against Gram negative aerobes, inactive against Gram positive anaerobes.tigemonamm is investigational Monobactam ms. (21) 4. CARBAPENEMS These βlactamm antibiotics have a 5 membered ring system which is fused to β lactam ring containing unsaturated carbon atom instead of sulphur atom which makes it different from Pencillin. It confers resistance to various β lactamases. Carbapenems are resistant to hydrolysis by most extended spectrum β lactamases and Amp C β lactamases. (15) E.g. Imipenem, Meropenem, Biapenem, Dorapenum, Ertapenem. GENERAL STRUCTURE OF CARBAPENEM 3.7. ANTIBIOTIC RESISTANCE Literature states that resistance β lactam antibiotics existed even before the introduction of first β lactam antibiotic. (13,20) Abram and Chain in 1940 identified bacterial Penicillinase even before the introductionn of penicillin as a therapeutic drug. (9) With the introductionn of antibiotic into general use, strains developedd mechanisms to inactivate the drug. Hence research was made to chemically modify penicillin to overcomee resistance. 13
25 Many genera of gram-negative bacteria possess β-lactamases which is chromosomally mediated. These enzymes are believed to have originated from Penicillin-binding proteins, with which they show some sequence homology. The selective pressure exerted by β-lactam-producing soil organisms would have led to the development of chromosome mediated beta lactamase. (20)(24) 3.6.GENETICS OF RESISTANCE Organism based resistance can be intrinsic or acquired. Intrinsic resistance resulting from normal structural physiological state of organism. (14)(16) Chromosomal resistance occurs as a result of mutation in a locus that controls susceptibility to given antimicrobial drug. The presence of antimicrobial drug serves as selective mechanism to suppress susceptible organism and favors growth of drug resistant mutant. Spontaneous mutation occur with frequency of 10 7 to and they are infrequent cause for emergence of clinical drug resistance. (16) Extra chromosomal: The plasmid genes for antimicrobial resistance control the formation of no. of enzymes that are capable of destroying antimicrobial drugs. Transposons and integrons are also involved in transfer of genes of drug resistance. (16) 14
26 Difference between two types of drug resistance Mutational drug resistance Chromosome mediated Resistance to 1 drug Non transferable Low degree of resistance Virulence of organism lowered Resistance is by altered metabolic pathway Transferable drug resistance Plasmid mediated Resistance to multiple drugs Transferable High degree of resistance Virulence not lowered Resistance is by production of degrading enzymes Transfer of drug resistance occurs by various mechanisms like conjugation through the agency of R plasmids [resistance plasmids].they carry 2 or more genes which encode variety of enzymes that degrade or destroy antibiotics. Resistance is also transmitted by transduction via agency of bacteriophage. (16) Transposons are small pieces of DNA that move from one site of bacterial chromosome to other site of chromosome or to plasmids and transmit resistance to many drugs. The expression of enzyme activity may be constitutive or inducible and may be expressed as homogenously or heterogeneously. (13) 15
27 3.8. MECHANISM OF ANTIBIOTIC RESISTANCE There is various mechanism of antibiotic resistance by which microorganisms destroy the antibiotic. (14) 1. Enzymatic inactivation 2. Altered drug target receptors 3. Alteration of antibiotic transport (efflux influx pumps) 4. Alteration of metabolic pathway The most common mechanism of resistance to β lactam antibiotics is by enzymatic inactivation. Bacterial resistance to β lactams may be mediated by various other mechanism like altering the antibiotic target, decreasing the intracellular uptake of the drug, but β lactamase production contributes as important mechanism of resistance in gram negative pathogens. (15)(4)(18) In the Gram negative bacteria,` β lactamases remain in the periplasmic space, where they attack the antibiotic before it reaches its receptor site. (24) In the Gram positive bacteria they are secreted to the outside membrane environment as exoenzymes BETA LACTAMASES PENCILLINASES These were the first beta lactamases identified. It was isolated by Abraham and Chain in E.coli even before pencillin entered clinical use. (18) β lactamases act by hydrolysing the β lactam ring leading to formation of pencilloic acid and by deacylation the enzyme reverts back to bind more pencillin molecules. (20) 16
28 Chromosomally mediated β lactamases are present in most of the genera of gram negative bacteria posses which is a natural phenomenon. This probably assists the bacteria in finding a way of protection when facing competition from other bacteria that naturally produce β-lactams. (23) In the early 1980s,third generation cephalosporins such as cefotaxime and ceftriaxone was developed and gained importance because of the increasing prevalence of Ampicillin-hydrolysing β-lactamases (TEM-1, TEM-2 and SHV-1) in Enterobacteriaceae, some respiratory pathogens such as Haemophilus influenza and Moraxella catarrhalis, and non-glucose fermenting Gram-negative bacilli. (19) A β-lactamase which hydrolyzed extended spectrum Cephalosporins was documented in strains of Klebsiella pneumonia in 1983,(Germany ),based on genetic and functional characteristics. Same findings were reported quickly from Europe and the US. They are called as extended spectrum β-lactamases because of their spectrum of activity against Oxyimino Cephalosporins. (23)(30) Currently, over 150 ESBL are known. In 1965, the first plasmid-mediated β-lactamasetem-1 was isolated in E.coli. (23)(39) The designation TEM came from the patient s name, Temoniera (20)(39). This occurred in a strain isolated from blood culture, from a patient in Greece. It soon spread to other members of the Enterobacteriaceae family, 17
29 Pseudomonas aeruginosa, Neisseria gonorrhea, and Haemophilus influenza, because this β lactamase was plasmid borne. SHV 1 (sulphydryl variable) is the second common plasmid mediated β- lactamase found in K. pneumoniae and E.coli. In K. pneumoniae the SHV1 β- lactamase is chromosomally encoded, but it is usually plasmid mediated in E. coli. (24)(39) The incidence and types of extended spectrum β lactamase enzymes varies with geographical location and time due to extended mutation. (24) Detection of these enzymes becomes utmost necessary in clinical practice ESBL These are group of β-lactamases which confer resistance to thirdgeneration cephalosporins and aztreonam, by hydrolysing the molecule. These are inhibited by clavulanic acids. (28) Mutations which alter the amino acid configuration around the active site of these β-lactamases, results in ESBL genes TEM-1, TEM-2, or SHV-1. ESBL pose a unique challenge to, Clinicians, clinical microbiologists, research scientists and infection control professionals face a challenge with ESBL. Numerous outbreaks worldwide are caused by Enterobacteriaceae that produce ESBLs. Unfortunately ESBL detection in the laboratory has become complicated by multiresistant bacteria. (19) These resistance is typically caused 18
30 by acquisition of plasmids containing genes which encode both ESBL, and other resistance genes. The most common β lactamase in GNB is TEM.TEM -1 production seems to be the common cause of Ampicillin resistance in E. coli I (>90%).Recently140 TEM type enzymes have been described BETA LACTAMASES CLASSIFICATION:- The basis of functional classification began when cephalosporinases, that had higher rates of hydrolysis for cephalosporins, has to be differentiated from Penicillinase, which hydrolyze only penicillin. (24) Several classification schemes were followed. It was based on molecular structure substrate profile, and location of genes. The first classification was developed by Richmond and Sykes followed by molecular class of Ambler. The Sykes classification was based on substrate profile and the location of gene. This Ambler classification separates beta lactamases to 4 distinct classes A to D based on similarities in amino acid sequence. (24) Class B is metallo β lactamases which require zinc atom for its activity. A C D act by serine based mechanism. Most important is class A which is serine proteases that have either preference for penicillin (or) broad spectrum activities. They are found either on chromosomes (or) plasmids and are easily transferable from one bacterium to another. They may be produced 19
31 constitutively and may be induced. In this group are the staphylococcus and some Gram negative bacilli. Class C: Primarily cephalosporinases, either constitutive (or) inducible, found on chromosomes of Gram Negative Bacilli. Class B & D are less important. The BUSH JACOBY system classifies beta lactamases according to functional similarities [substrate and inhibitor profile] (25) Group 1 Cephalosporinases that are not inhibited by clavulanic acid Group2 Pencillanases, Cephalosporinases, and broad spectrum β lactamases that are generally inhibited by beta lactamase inhibitors Group 3 Metallobetalactamases that hydrolyses Pencillins, Cephalosporins, and Carbapenems. ESBLs belong to group 2be which are enzymes derived from 2b, denoting a broad spectrum of action or 2d OXA type with similar activity but differs by being resistance to clavulanic acid. (28) More than 890 β lactamases are reported; the largest occurred in class A class D families. To illustrate, there are currently more than 165 TEM β lactamases, 75 ESBL s of TEM family, 36 inhibitor resistant TEM, 126 SHV, OXA 160 enzymes and 91 CTX M ESBL. Classification table is attached in Annexure-I. 20
32 3.12ESBLs - Epidemiology Enterobacteriaceae producing ESBL strains is a challenge in treating hospitalized as well as community based patients. Production of ESBL began in Europe, however within few years it spread to United States and Asia. It varies from 6% to 87% from previous studies in India. The uniqueness of ESBL is its specificity. A prospective study on antibiotic co resistance and ESBL in urinary isolates from North East India has noted the ESBL detection rate as 24.56%. A study from New Delhi showed per cent of the strains of Gram negative bacteria as ESBL producers. (72) Ritu Agarwal et al from Pune in their study on prevalence of ESBL among E.coli and Klebsiella pneumoniae isolates found that 40% of E.coli and 54.5% of Klebsiella pneumoniae were ESBL producers. (73) Pushpa D et al from Amristar, Punjab has found ESBL production among 43.83% of their uropathogens. Tankhiwale et al from Nagpur detected 48.3% of uropathogens to be ESBL producers. (71) They also found 90.5% of the ESBL producing isolates were multi drug resistant. ESBL production was detected in about 36% of K. pneumoniae and 47% of E.coli infections in a study from Chennai suburban. (49) From Mangalore ESBL was reported as 39.5% in a study by Eshwar Singh. (39) CTX M beta lactamases CTX M. is the second largest group of ESBL which shows greater activity against Cefotaxime than other oxyimino beta lactam substrate [Ceftriaxone, Cefepime Ceftazidime]. (24) they are plasmid acquired genes of beta lactamases which were previously found on the chromosome of kluyvera 21
33 species. These enzymes are classified to 5 major groups, based on Amino acid sequences. CTX- M1 cluster has been related to chromosomal bla gene present in different Kluyvera cryocrescens CTX- M2 cluster originates from gene KLU A OF Kluyvera ascorbata. The other clusters have genes originated from Kluyvera Georgina. (20) OXA BETA LACTAMASES These belong to molecular class D and functional group 2d.Hydrolytic activity to oxacillin and cloxacillin is high but action against clavulanic acid is poor. It acquires the ESBL phenotype by amino acid substitution in OXA enzymes. [20] INHIBITOR RESISTANT β lactamases Among E. coli beta lactamase that were not resistant to clavulanic acid was discovered in early 1990 s and were termed as inhibitor resistant β lactamases. Though they are not ESBL s, since they are derived from classical TEM SHV enzymes, they are discussed along with ESBL. (20) There are at least 19 distinct enzymes found mainly in E.coli and few strains of Klebsiella pneumonia.they are susceptible to inhibition to Tazobactam Amp C betalactamases: Class C Amp C beta-lactamase are Ambler class C or group I cephalosporinases that confer resistance to cephalosporins and cephamycin and are not affected by inhibitors (Tazobactam, Clavulanic acid and Sulbactam). (32) 22
34 Their ability to hydrolyse cephamycin as well as other extendedspectrum cephalosporins differentiates them from other extended-spectrum β- lactamases (ESBLs) (30). These are mostly chromosomal beta lactamases and are produced to greater or lesser extent by almost all GNB. Of the two types of Amp C (plasmid-mediated and chromosomal), the former is encountered in Klebsiella species, Proteus mirabilis and Salmonella species while the latter is seen in organisms such as Morganella morganii, Enterobacter cloacae, Citrobacter freundii, Hafnia alvei and Serratia marcescens. Escherichia coli is unique in that it also expresses chromosomal Amp C at low levels. (32) The widespread distribution of Amp C genes on transmissible plasmids is a continuous challenge for research people. Bacteria lacking chromosomal bla Amp c gene acquired it from transmissible plasmids. Amp C enzymes are inducible in many bacteria and can be expressed at high levels, by mutation. Boronic acid and cloxacillin inhibit Amp C β lactamases. (29)(30) E. coli, Enterobacter cloacae, S. marcescens, Pseudomonas aeruginosa and Citrobacter freundii possess chromosomal sequences which encode β lactamases of the AmpC type. This β-lactamase which is a product of the AmpC gene is broadly active against Cephalosporins but is not inhibited by Clavulanic acid, thus differs from ESBLs. (31) 23
35 Chromosome-encoded AmpC is usually an inducible enzyme that is expressed at low basal levels, but in some species such as E. coli, the enzyme is non inducible. (30) (20). Beta-lactam antibiotics, such as Cefoxitin, Cefotetan, and Imipenem, induce the expression of AmpC genes which are chromosomally located and mediated by the regulator AmpR. The most common cause of constitutive hyper production of AmpC beta-lactamases is mutation in the repressor gene AmpD. (41) Numerous pathogens produce plasmid-encoded AmpC β-lactamases, e.g. Salmonella spp, Citrobacter freundii, Klebsiella pneumoniae, Escherichia coli, and Proteus mirabilis They are separated to 4 groups: GROUP 1 plasmid encoded Amp C cephalosporinases consist of those which originated from Amp C of Citrobacter freundii. GROUP 2 are related to chromosome Cephalosporinases of E. cloacae. GROUP 3 are from Amp C of Pseudomonas GROUP 4 CMY beta lactamases At present there are no CLSI or other approved criteria for detection of Amp C β lactamase. A positive ESBL screening test, and a negative confirmatory test involving increased sensitivity to clavulanic acid is typical of organism producing enough Amp C β lactamase. (29) 24
36 Treatment of infection with Amp C strains is difficult as most Pencillins and Cephalosporins are ineffective. Cefepime can be used. Imipenem, Ertapenem or Temocilin are found to be active. Fluoroquinolone therapy and Tigecycline is another option for treatment. Hence in clinical management, recognition of Amp C producing E.coli strain is important as in therapeutic failure occurs often on administration of β lactam drugs. (50) CARBAPENAMASES These are versatile beta lactamases encoded by plasmids which hydrolyze Pencillin, all third generation Cephalosporins, Carbapenems like Imipenem, Meropenem, and Doripenem. (43) They are more stable than extended spectrum β lactamases and Amp C β lactamases. Plasmid mediated MBL genes should be detected at the earliest as they spread rapidly to other gram negative bacteria. This makes necessary for the modification of therapy and initiation of effective infection control. Recently Metallo- Beta-lactamases (MBLs) has emerged as the most problematic resistance mechanisms because they hydrolyze all beta lactams including carbapenems except Aztreonam. (36) They are inhibited by EDTA chelators (19) The first metallo lactamases which were initially studied were chromosomal enzymes. These were detected in Bacillus cereus, Aeromonas 25
37 spp. and Stenotrophomonas maltophilia, which are environmental and opportunistic pathogenic bacteria. (43) Among Enterobacteriaceae, 1st carbapenamase enzyme (bla) IMP-1was discovered in 1991 in Serratia marscences in Japan, which was followed by reports from Greece and United States on identification of bla VIM, bla KPC (8)(43). MBL genes seem to have disseminated from Pseudomonas aeruginosa to other members of family Enterobacteriaceae. Worldwide prevalence of MBL is seen with Pseudomonas aeruginosa and also recently among Gram negative bacilli. (43) As the MBL genes are present in mobile gene cassettes, which are inserted in integrons the resistance may spread rapidly to various species of gram-negative bacilli. Thus there is a need to detect MBL in gramnegative bacilli rapidly in order to prevent dissemination and thereby helping in infection control. (37) The infection with these MBL strains still remains a nightmare for clinicians in treating organisms. These MBL strains can lead to increased mortality and morbidity. There are two types by which these enzymes act, either by serine based mechanism or requiring zinc or metal chelators for their action. Class A D act by are serine based hydrolytic mechanism SME KPC, IMI NMC SME GES families. Some are chromosomal, (SME, IMI- 1) others are plasmid encoded (GES KPC, IMI-2). All hydrolyze carbapenems and they are partially inhibited by clavulanic acid. 26
38 Class B are Metallobetalactamases [MBL] which require zinc for their activity.( IMP, VIM, SPM, GIM, SIM, NDM -1.)These hydrolyze all beta lactams including Carbapenem, Extended Spectrum Cephalosporins, except Aztreonam. They are inhibited by chelators like EDTA. KPC - IMP - KPC - VIM - NDM - Klebsiella pneumoniae beta lactamases Imipenamase metallo beta lactamases Klebsiella pneumonia carbapenamase Verona integron encoded metalloβ lactamases New Delhi metalloβ lactamases originally discovered from New Delhi in 2009 in a Sweedish patient of Indian origin, who acquired urinary tract infection.this gene is now found in many species of E. Coli and Klebsiella from places in India and Pakistan. (37) Class D: These are OXA type β lactamases. The chromosomal gene of Shewanella spp, that moved through plasmid to Enterobacteriaceae, these are not inhibited by Clavulanic acid or EDTA. It was first reported in Turkey. 34 several reports have shown that MBL carrying organism may be susceptible to Carbapenem (in vitro) but actively resistant in vivo (Clare et al 2006, Pelg et al 2005). 27
39 3.18.LAB DIAGNOSIS OF ESBL PHENOTYPIC DETECTION METHODS OF ESBL To detect ESBL several phenotypic tests was developed since 1980s utilizing the two characteristic features of ESBL. (35) a) Decreased susceptibility to Cephalosporin b) Inhibition by Clavulanic acid CLSI (2014M100-SS24) recommends disc diffusion method to screen ESBL among Klebsiella, Escherichia coli and phenotypic confirmatory test for confirmation : SCREENING TESTS FOE ESBL Disc diffusion method with indicator Cephalosporin of III generation Ceftriaxone (30 μg/disk): 25 mm, Cefopodoxime (10μg /disk): 17 mm; Ceftazidime (30 μg/disk): 22 mm; Cefotaxime (30 μg/disk): 27 mm; Susceptibility testing was performed on Mueller-Hinton agar using McFarland 0.5 standard from overnight cultures, followed by incubation at 35 C for 16 to 18 hours. Zone diameters and MIC range of various antibiotics Sensitive Resistant Antibiotic(μg) Disc diffusion(resistant) MIC MIC Cefotaxime(30) 27mm 1μg/ml 4μg/ml Ceftazidime(30) 22mm 4μg/ml 16μg/ml Aztreonam(30) 27mm 4μg/ml 16μg/ml Ceftriaxone(30) 25mm 1μg/ml 4μg/ml 28
40 For Pseudomonas species, the ceftazidime resistance is considered when zone diameter is 14 mm and sensitive if it is 18 mm. while doing MIC, resistance is confirmed when if it is greater than 32 μg (11) : Confirmatory test: Double disc diffusion test Combined disc test Broth micro dilution test/agar microdilution Three dimensional test Agar supplemented with clavulanate E test Automated system (Vitek test / microscan panel / BD phoenix automated system) CONFIRMATORY TESTS Double disc diffusion test (11) The test innoculum is spread as lawn culture on Muller Hinton agar plate using sterile cotton swab. Disc of ceftazidime (30μg) and clavulanic acid (10μg) was placed on the surface of MHA, and then the disc of ceftazidime (30μg) was placed at distance of 15 mm from previous disc. The inoculated plates were incubated overnight in the incubator and the zone of inhibition between discs is compared. They are said to be ESBL producers when zone diameter difference is greater than 5mm. 29
41 Double disc synergy test The innoculum of the organism to be tested is spread on MHA plate using cotton swab which should be sterile. The disc of ceftazidime is placed at distance of 30 mm from Amoxyclavdisc, and incubated overnight hours, and enhancement of zone of inhibition towards clavulanic acid is suggestive of ESBL production. (28) Implications of positive phenotypic confirmatory tests: As per CLSI guidelines, isolates tested positive by confirmatory test are reported as resistant to all cephalosporins and Aztreonam, excluding Cefoxitin, Cephamycin and Cefotetan, irrespective of their individual MICs. MIC determination :It is done by Broth or agar microdilution method Done by agar dilution method Preparation of media: Muller Hinton agar was prepared in tubes and autoclaved. It is then allowed to cool in a 50 o C water bath. Serial dilution of the 3 rd Generation Cephalosporins, Ceftazidime and Meropenem is prepared in sterile distilled water to give a final concentration ranging from 2μg 128μg/ml of agar. After adding the drugs to the medium at 50 o Cit is mixed well and poured into sterile Petri dishes. The media was used immediately otherwise potency of drugs will be affected. We can inoculate upto 20 different organisms in a single plate. A 30
42 control plate containing the test medium without the antibiotic was prepared for each series of test. Innoculum Preparation: Isolates belonging to same morphological type (at least 3-4) were selected from an agar culture plate. These are transferred to a tube containing4-5ml of broth. The broth culture was incubated at 37 o C till it the required turbidity i.e. 0.5 McFarland s standard (usually 2-3 hours) is obtained. Inoculation of test plates: Plates of various concentrations were divided into required number (15-20 divisions / plate) ml of innoculum was put into the appropriate quadrant and incubated at 37 o C for hrs. Minimum inhibitory concentration was the lowest concentration at which no visible growth occurs. Quality Control used for ESBL detection: The positive control used was Klebsiella pneumoniae ATCC and negative control was Escherichia coli ATCC Commercially Available Methods for ESBL Detection: (i)e test for ESBLs This is a useful test in the diagnostic armamentarium. It consists of antimicrobial agent impregnated plastic strips, produced by AB Biodisc (Solna, Sweden) placed on surface of agar. The principle is expansion of disc diffusion method. Various gradients of ceftazidime are printed linearly on the strip 31
43 .Elliptical zone of inhibition is taken as positive. The test is done in the presence Clavulanate impregnated on other side along with Ceftazidime. The 8-fold reduction in MICs of Cephalosporin is considered as positive as per manufacture guidelines. 95 to 100%. Sensitivity reported for this method is 87 to 100% and the specificity is Automated methods (ii)vitek ESBL cards: This test utilizes Cefotaxime and Ceftazidime, alone (at 0.5 μg/ml), and in combination with Clavulanic acid (4 μg/ml). After 4 to 15 hours of incubation once the growth control well has reached a set threshold, the readings are automatically analyzed. The cards are inoculated identical to that performed for regular Vitek cards. Once analysis of all wells is performed, positivity is recorded by comparing the two wells.when there is reduction in the growth of the Cefotaxime or Ceftazidime wells containing Clavulanic acid, compared with that of growth in the well with the cephalosporin alone, it indicates a positive result. Sensitivity and specificity of the test are remarkable. Molecular ESBL detection techniques: There are several molecular biological methods to characterize organisms. Detection of specific nucleic acid sequences by hybridization with DNA probes for TEM or SHV enzymes. 32
44 PCR- It is an-vitro technique to replicate specific sequence of DNA. It amplifies a DNA target by repetition of a basic cycle by using specific prime RPLF- It is based on the detection of base pair changes at restriction sites. Nucleotide sequencing is the gold standard for determining specific beta lactamase gene LAB DETECTION OF CARBAPENAMASES Different studies suggest different methods to detect MBL production as there is no standard set of guidelines. Detection of carbapenamase is complicated because some carbapenamase producing isolates demonstrate elevated but susceptible carbapenem MICs : Screening tests: Zone diameter and MIC for Enterobacteriaceae Antimicrobial agent(μg) Disc method(mm) Resistant Intermediate Sensitive MIC(μg) (sensitive) Ertapenem(10) Imipenem(10) Meropenem(10)
45 Zone diameter and MIC for Pseudomonas Antimicrobial agent(μg) Disc method(mm) Resistant Intermediate Sensitive MIC sensitive(μg) Ertapenem (10) Imipenem(10) Meropenem(10) CONFIRMATORY TESTS Confirmation of carbapenamase production is done by confirmatory tests : PHENOTYPIC DETECTION TEST DOUBLE DISC SYNERGY TEST COMBINED DISC TEST MODIFIED HODGE TEST MIC E TEST MOLECULAR METHOD Confirmatory tests are carried out to detect MBL production in Imipenem resistant cases. This is done by combined disc test with Imipenem and EDTA. This method that is highly sensitive and specific at detecting both carbapenem-susceptible (98.33%) and carbapenem-resistant MBL-carrying isolates among the gram-negative genera. The selection for phenotypic MBL detection is more challenging with the emergence of carbapenem-susceptible 34
46 MBL-carrying organisms; therefore, screening only carbapenem-resistant organisms, as is mostly performed by clinical laboratories is suboptimal. [2](74) Hence detection of MBL in all isolates is advocated. MODIFIED HODGE TEST (10) To detect carbapenamase, E.coli ATCC lawn culture is done on MHA. Imipenem disc (10μg) is placed in the centre. The strains were streaked from the periphery of the centre disc on all sides. The plate was incubated for 18 hours incubation. Enhancement of growth of indicator strains around Imipenem disc is taken as Modified Hodge test positive. No enhanced growth is taken as negative for carbapenamase production. The appearance of clover leaf pattern is diagnostic. In Remodified Hodge test Imipenem plus zinc disc is used zinc has known to increase metallo beta lactamases activity. DETECTION OF MBL BASED ON INHIBITION OF CHELATING AGENTS : This is specific test based on using the chelating agents which has inhibitory effect on MBL. These compounds inactivate MBL that act against beta lactams, depriving them of the hydrolytic essential Zn 2+ cat ion. The DDST and CDT are commonly used forms of MBL detection. IMIPENEM EDTA DISC TEST The MHA plate is inoculated with the test organism by sterile cotton swab, an Imipenem disc (10 μg) is applied over it, another disc of Imipenem and EDTA is placed at distance of 15 cm is placed on the MHA plate. The 35
47 plate is incubated for hours. A difference in zone diameter of > 7 cm between two discs is indicative of metallo betalactamases production. Imipenem/Ceftazidime double disc synergy test (DDST): Test organisms inoculated on to plates with Muller Hinton agar following CLSI recommendations.an imipenem (10 μg) disc placed 20 mm centre to centre from a blank disc containing 10 μl of 0.5 M EDTA (750 μg). Positive result is interpreted if the area between Imipenem and clavulanate shows enhancement in comparison with the zone of inhibition on the other side of the disc. MBL E-test: This is a quantitative method of detecting MIC by using the principles of both dilution and diffusion of antibiotic into the medium. It contains an absorbent strip containing predetermined gradient of IPM (4 to 256 μg/ml) and IPM (1 to 64 μg/ml) in combination with a fixed concentration of EDTA on the other side. It is reported to be the most sensitive test for MBL detection. The Etest is done according to manufacturer's instructions. MIC ratio of IP (Imipenem)/IPI (Imipenem-EDTA) of >8 indicates MBL production. The MIC concentration at which the ellipse intersects at the strip is the MIC value. (13) MOLECULAR METHODS: The reference standard for precise identification of carbapenamase is by molecular technique where the gene for resistance is identified. Most of these techniques are based on hybridization techniques. Their cost and the 36
48 requirement for trained microbiologists limit their routine utility. Several multiplex real time PCR methods and other newer methods are available. 3.20: LAB TESTS FOR AmpC DETECTION There are no universally approved criteria for AmpC detection even by CLSI. Organisms producing enough AmpC β-lactamase will typically give a positive ESBL screening test but the confirmatory test will be negative and shows sensitivity with clavulanic acid. (32) : SCREENING: Resistance to cefoxitin (zone size < 18 mm) as well as oxyimino cephalosporins suggests Amp C enzyme production. (11) CONFIRMATION TESTS Three dimensional tests Cefoxitin agar Amp C disc test Inhibitor based tests: using Ro LN 2-128, SYN 2190, CLOXACILLIN Boronic acid, Phenyl boronic acid, 3 Aminophenylboronic acid THREE DIMENSIONAL TESTS Standard E. coli strain (ATCC 25922) is streaked on MHA, a circular hole in the agar was cut near about 3mm from the disc cefoxitin. The suspension of test organism is added to the well. Distortion of zone at the point 37
49 of cut in the agar indicated the presence of enzyme. (13) It is most sensitive method but technically more demanding to perform. MODIFICATIONS A radial slit was employed,rather than using intact cells,the test organism were concentrated by centrifugation and the pellet was freeze thawed 7-8 times to release β lactamases. A heavy innoculum streaked radially from cefoxitin disc on agar surface without using slit. CEFOXITIN AGAR: The agar plate containing 4 μg / ml of Cefoxitin is streaked with the sensitive indicator strain. To a well in the plate, freeze thawed cell extract of test organism is added. After incubation presence of growth around the well indicates Cefoxitin hydrolysing enzymes. The advantage of this method is that it is easier to perform, allows multiple samples to be tested per plate and as sensitive as three dimensional test,. (29) Amp C disc test. This is a rapid test for detection of Amp C. This is otherwise known as Tris EDTA test. Here, E. coli culture (ATCC 25922)was swabbed on MHA plate. A cefoxitin disc was placed.sterile disks (6 mm) were wetted with sterile saline and inoculated with several colonies of test organism. This disc was then placed beside the cefoxitin disk (almost touching). The plates were incubated overnight at 35 C. A positive test appeared as a flattening or 38
50 indentation of the cefoxitin inhibition zone in the vicinity of the test disk. A negative test had no distorted zone. (42) It is simple, and convenient to perform. Phenotypic confirmation testing of AmpC The Etest for AmpC is confirmatory. The test principle comprises a strip impregnated with a concentration gradient of Cefotetan on one half of the strip and Cefotetan with Cloxacillin on the other half of the strip. MICs of Cefotetan alone and Cefotetan with Cloxacillin were determined as recommended by the manufacturer. (41) A 8 fold reduction between the two is taken as positive. Inhibitor based tests: The use of inhibitors to detect AmpC is similar to confirmatory test for ESBL using Clavulanic acid. Boronic acid and cloxacillin are usually used. They inhibit Amp C enzymes and potentiate the action of cephems. (78) Cefoxitin-cloxacillin double disc synergy test (CC-DDS) Cefoxitin discs of 30 μg and Cefoxitin plus Cloxacillin (30μg/200μg) were used. The strains were inoculated on Mueller-Hinton agar using McFarland 0.5, and incubated overnight at 35 C. The inhibition zones of Cefoxitin-Cloxacillin and that of Cefoxitin zones are compared. A 4mm difference in zone is indicative for AmpC production. (41) 39
51 BORONIC ACID Various boronic acid derivatives are added to blank βlactam disc which is placed near unmodified beta lactam disc for comparison. Disc potentiation > 5 mm zone of inhibition in boronic acid disk is taken as positive. (29) Several other studies evaluated the β-lactams enzyme inhibitors LN-2-128, Ro , and Syn 2190combination with Cefotetan, gives the best results, which was 100% specific and 91% sensitive in AmpC β-lactamase detection. Unfortunately, these inhibitors are not commercially available. (39 ) The inhibitor-based test showed the potential for the detection of organisms producing plasmid mediated Amp C βlactamases by using cefotetan in combination with LN and LN and are inhibitors of class A -lactamases in addition to AmpC β lactamases. A novel AmpC β-lactamase inhibitor, Syn 2190 does not inhibit class A lactamases. However LN which is a C-3-substituted cephalosporin-derived inhibitor with a broad spectrum of inhibition and inhibits both class A (e.g., TEM and SHV) and class C (e.g., AmpC) lactamases. (40) A positive test for a plasmid mediated Amp C β lactamase is accepted when >4mm increase in zone diameter in present with inhibitor and plain antibiotic alone. MOLECULAR METHODS: PCR : using Multiplex PCR assay six family of genes, can be identified 40
52 REAL TIME PCR: DNA probes It reduces the reporting time. Specific for gene family are available ( e.g. MOX, DHA, EBC,ACC, FOX,, CIT, ) BETA LACTAMASE INHIBITORS: These are compounds which resemble β-lactam antibiotics. They can bind to β-lactam antibiotics either reversibly or irreversibly protecting the antibiotics from destruction. They serve as suicide bombers utilizing all available enzymes. These have weak antimicrobial activity but have potent inhibitor effect on many plasmid-encoded and some chromosomal β- lactamases. Three important β-lactamase inhibitors are: 1) Clavulanic acid 2) Sulbactam 3) Tazobactam 41
53 Materials and Methods
54 MATERIALS AND METHODS A prospective study was conducted from April 2014 to March 2015 in the department of Microbiology, Karpaga Vinayaga Institute of Medical Sciences and Research Centre, Kancheepuram district. The present study aims to find out the various β lactamases producing gram negative bacteria from the samples received from outpatients and inpatients, who were admitted to different wards in our hospital. 492 Gram negative bacilli (GNB) were isolated from various clinical specimens, from April 2014 to March ETHICAL CONSIDERATION: Ethical committee of Karpaga Vinayaga Institute of Medical Sciences and Research centre gave the Ethical clearance for the study. METHODOLOGY Isolates obtained from various clinical samples sent to the microbiology laboratory were identified by standard microbiological techniques. The antimicrobial susceptibility testing was carried out by the disc diffusion method by Kirby Bauer according to CLSI guidelines. Antimicrobial discs [Himedia Mumbai] used were: Amikacin (30ug), Ampicillin (10 µg), Amoxicillinclavulanic acid (30/10μg), Gentamicin (10ug), Ciprofloxacin (5µg), Cotrimoxazole (1.25/23.75µg) Ceftriaxone (30 µg), Cefotaxime (30µg), Ceftazidime (30µg) and Imipenem (10µg). Quality control was achieved by using E.coli ATCC The isolates showing resistance to any of the 3GC 42
55 were stored in stock vials for further processing. Media and disks were tested for quality control with standard strains. INCLUSION CRITERIA 1. All gram negative clinical isolates from both sexes of all age group were included in the study. 2. Enterobacteriaceae and Nonfermenters showing resistant to any of the third generation cephalosporins were tested for beta lactamase production (ESBL, Amp C and Carbapenamase) EXCLUSION CRITERIA 1. Non Enterobacteriaceae isolates were excluded. 2. Those samples which showed mixed growth were excluded 3. Isolates sensitive to all antimicrobial disc tested were excluded The isolates stored in the stock vials were sub cultured at the time of testing. The purity and viability of the isolates was checked. They were subjected to various phenotypic methods of β lactamases detection along with MIC determination. Agar dilution technique was used for MIC was determination. Preparation of Innoculum: Similar looking 3 to 5 representative colonies were touched with a sterile wire and inoculated in 4-5ml of broth (peptone water) and incubated at 37 o C for 2 6 hrs till 0.5 McFarland s standard is attained. If the broth is more turbid then some more broth was added under 43
56 sterile condition and to match 0.5 McFarland s standard. Inoculation of MHA plates was made within 15 minutes by using sterile cotton swab. Excess broth from the swab was removed by pressing firmly sidewall of the tube and Inoculation in Muller Hinton agar plate was done. To ensure even distribution of the innoculum, the procedure was repeated by turning the plate to about 60 0 angle each time and finally the rim of the agar was streaked. The standard predetermined set of antimicrobial discs were placed on the agar plates and pressed adequately so that the disc has firm contact with the agar surface. The distance between the antibiotic discs should at least 24 mm from centre to centre of the discs. Inoculated plates were inverted and incubated at 37 o C for hrs. Those specimens which showed resistance to one of III generation cephalosporins was subjected to other tests for detection of ESBL, Amp C, and Carbapenamase production. Detection of the ESBLs Phenotypic tests were done to confirm ESBL i.e. combined disc test which uses Ceftazidime [30μg] and Ceftazidime-clavulanic [30/10μg discs). Detection of the Amp C β-lactamases: Cefoxitin disc was used for Amp C detection among the isolates. Those which showed Cefoxitin zone of inhibition 18 mm were taken as Amp C positive. 44
57 Then resistant isolates (Cefoxitin resistance) was subjected to Amp C disc test. The AmpC production is indicated by an indentation or a flattening of the zone of inhibition. (7) Detection of the Carbapenamases: The carbapenamase production was detected by the Modified Hodge test and Imipenem EDTA combined disc test. Clover leaf pattern in Modified Hodge test was taken as positive. The organisms were considered to be MBL producers if the increase in the zone of inhibition between Imipenem and Imipenem EDTA (10μg/750μg){Himedia} disc was 7mm in combined disc test. DETECTION OF ESBL Combined disc test (Phenotypic Confirmation Test) Growth of the organism was obtained as lawn culture. A Ceftazidime (30µg) disc alone and its combination with 10mg of clavulanic acid was placed on the plate at distance of 15 mm.the inoculated plates were incubated at 35 0 C in the incubator for hours. When there was 5mm increase in zone of inhibition between ceftazidime / clavulanic acid (30µg/10µg) and plain Ceftazidime are confirmed as ESBLs producers as per CLSI guidelines. (11) 45
58 Detection of Amp C Amp C disc test. (64) Isolates showing resistant to Cefoxitin (30μg) were subjected to Amp C disc test. Here, ATCC E coli was used as a lawn culture. The Cefoxitin disc was then placed and beside it a sterile disc, {Whattman No. 1 filter paper (6 mm) size} wetted with sterile saline and inoculated with several colonies of test organism and placed almost touching. The plates were incubated overnight at 35 C. A positive test appeared as a flattening or indentation of the Cefoxitin inhibition zone in the vicinity of the test disc. A negative test had an undistorted zone. Detection of Carbapenamase production Modified Hodge test (11) Lawn culture of E.coli ATCC was done on Mueller Hinton agar plate. Imipenem disc (10μg) was placed in centre of the culture plate. Four test strains were inoculated from periphery of the disc on all sides. Following incubation, enhancement of zone of inhibition of growth indicator strains around Imipenem is taken as Modified Hodge test positive. Combined Disc test Lawn culture of test isolate was made on Mueller Hinton agar plate. A Imipenem disc (10 μg) was placed on MHA plate, another disc having Imipenem and EDTA(10/750μg) was placed with a of distance of 15 mm from the Imipenem disc. The plates were incubated at 37 0 C in incubator. MBL 46
59 production was taken as positive if the zone of inhibition is >7mm between the two discs. PCR for detection of resistance genes: DNA EXTRACTION: DNA was extracted from the selective isolates using DNA purification kit (Pure Fast Bacterial Genomic DNA purification kit). (Helini Biomolecules). The procedure is attached in Annexure II. The following were the primers used HELINI TEM gene primer Forward Primer: 5'-GATAACACTGCGGCCAACTT -3' Reverse Primer: 5'-CTGCAACTTTATCCGCCTCC PCR-3' Product size: 262bp HELINI -SHV gene primer Forward Primer: 5'-CGCCGCCATTACCATGAGCGAT -3' Reverse Primer: 5'-ACCCGATCGTCCACCATCCACT PCR-3' Product size: 276bp HELINI -IMP gene primer Forward Primer-5'-TTTTGCAGCATTGCTACCGC-3' Reverse primer-5'-cacgctccacaaaccaagtg-3' Product size = 220bp 47
60 STATISTICAL ANALYSIS: The observations of the study were recorded and analyzed. The results were compared and discussed by using SSPS software and Chi Square test 48
61 Results










62 5. RESULTS 492 gram negative samples were obtained during the study period (April 2014 to March 2015), among which 204 isolates showing resistance to one of the III generation cephalosporins, were taken for beta lactamase detection. 5.1: Age wise distribution of isolates: The specimens received were from various age groups, predominantly falling in the age group of years (44.12%), as shown in fig >60 Fig 1: Age wise distribution of isolates 49

 107 108 106 104 102 1000 97 98 96 94")



63 5.2: Sex wise distribution of isolates: The clinical isolates were obtained from 97 male patients and 107 female patients. (Fig 2) Male Female Fig 2: Sex wise distribution of isolates 5.3: Distribution of isolates: Among 204 resistant clinical isolates, 174 isolatess were from IP and 30 were from OP. Table 1 : Distribution of isolates Total strains OP Percentage IP Percentage % % 50
64 5.4: Specimen wise distribution of isolates: The various clinical specimens from which these isolates were obtained are as follows- urine (100), pus(58), sputum( 30),wound swab (4), cervical swab (2), high vaginal swab(2), aural swab(1), catheter tip (3), tracheal tip(1),tissue(2) and blood (1). The results are shown below. Specimens Table 2: Distribution of isolates in samples No. of samples (n=204) Percentage % Urine Pus Sputum Wound swab Cervical swab Catheter tip Tissue High vaginal swab Aural swab Blood Tracheal tip Total In our study the urinary tract infections were predominant 49.01%, (100/204),followed by skin and soft tissue infections 30.4% {pus samples 58/204 and wound swab 4/204} and respiratory infections was 14.71%. (30/204) 51
65 5.5: Ward wise distribution: Among the 204 samples 174 samples were from inpatients, in which 44 were from ICU and 142 were from various wards. The number of isolates from each ward was as follows:19 from male medical ward, 16 from female medical ward 38 from male surgical ward,18 from female surgical ward 6 from pediatric ward, 32 from Gynecology ward, 1 from ENT ward and 30 from OPD as shown in Table :3. Table:3:Samples collected ward wise Wards No. of samples (n=204) Percentage% ICU % Male medical ward % Female medical ward % Male surgical ward % Female surgical ward % Gynecology % Pediatrics % ENT % OPD % The maximum number of samples were from inpatients % followed by OPD 14.71%. In IP maximum numbers of samples were received, from ICU and male surgical ward as % and 18.62%respectively. 52
66 5.6: Distribution of samples in various wards Samples were received from various wards whose distribution is shown below. Table: 4: Distribution of samples in various wards. Ward Urine Pus Sputum Wound swab Others ICU MSW GYNAEC MMW FSW FMW PAEDIATRIC ENT OP TOTAL :7: Number of GNB isolated: Among the 204 isolates, 161 isolates belong to family Enterobacteriaceae and nonfermenters constituted 43 isolates. Out of the 161, 105 samples showed growth of E.coli, 51 had Klebsiella species, 02 were Enterobacter species and 03 were Citrobacter species. Among the nonfermenters, 37 were Pseudomonas species and 06 belong to Acinetobacter species. 53
67 Table 5 : Number of GNB isolated Organism Number Percent E.coli % Klebsiella spp % Pseudomonas spp % Acinetobacter spp % Citrobacter spp % Enterobacter spp % Total % The commonest gram negative isolate among the isolates was E. coli which was found in 105 (51.47%) samples, followed by Klebsiella in 51 (25%) and Pseudomonas in 37 (18.14%). 5.8: Distribution of isolates in various wards: Ward wise distribution of isolates are shown in Table 6. Table 6 : Distribution of isolates in various wards E.coli Isolates Medical Surgical Klebsiella spp. Pseudomonas spp. Acinetobacter spp. Citrobacter spp. Enterobacter spp. 19 (54.3%) 5 (14.3%) 9 (25.7%) - 2 (5.7%) - 22 (38.6%) 17 (29.8%) 11 (19.3%) 3 (7%) 1 (1.7%) 2 (3.5%) Gynae cology 17 (53.1%) 8 (25%) 6 (18.8%) 1 (3.1%) ICU 22 (48.9%) 14 (33.3%) 7 (15.6%) 1 (2.2%) Pae Diatric 5 (66.7%) 1 (22.2%) - - OP 19 (63%) 06 (20%) 04 (10%) 01 (3.3%)
68 E.coli was the common organism isolated among the samples from various wards. In the medical ward the common organism isolated was E. coli (54.3%) followed by Pseudomonas spp. (25.7%). It was observed that E.coli was also common organism among the specimens of surgical wards (38.6%) and ICU (48.9%). Klebsiella species was the second common isolate in ICU specimens (33.3%) and in surgical wards (29.8%). Pseudomonas spp. was almost equal among the specimens from various wards in IPD except in Pediatric ward which showed the least number of isolates. 5.9: Clinical specimen and organism isolated: The organism isolated from various clinical specimens is showed in table 6. Table 7: Clinical Specimen and Organism isolated Samples E.coli Klebsiella Pseud monas Acineto bacter Citro bacter Entero bacter Urine(100) 76(76%) 14 (14%) 07(7%) - 01(1%) 02 (2%) Pus(58) 21(36.2%) 20(34.5%) 12(20.7%) 03(5.2%) 02(1.7%) - Sputum(30) 02(6.7%) 12 (40%) 14(46.7%) 02(6.7%) - - Wound Swab(4) 02 (50%) 2 (50%) HVS(2) 01 (50%) 01 (50%) Cervix swab(2) 01 (50%) - 01 (50%) Catheter tip(3) 01(33.3%) - 01(33.3%) 01(33.3%) - - Blood(1) 01 (100%) Aural swab(1) (100%) Tissue(2) - 01 (50%) 01(50%) TrachealTip(1) - 01 (100%)
69 E.coli was most common organism isolated from urinary samples 76/105 (76%), followed by Klebsiella spp. 14/100 (14%). In pus samples E.coli constituted (36.2%) and Klebsiella spp. 34.5%. In sputum samples Klebsiella spp. and Pseudomonas spp. were almost equal, 40% and 46% respectively. 5.10: Antibiotic susceptibility pattern: The antibiotic susceptibility test was done by Kirby Bauer technique to determine the susceptibility pattern of isolates which are shown below in Table 8. The interpretation was done according to CLSI guidelines Antibiotics dose (μg) Table 8: Antibiotic susceptibility pattern Clinical isolates n=204 Sensitivity Percentage Ampicillin (10) % Amoxy clav(20/10 ) % Cotrimaxole(1.25/23.75) % Ciprofloxacin(5) % Nitrofurantoin(10) % Gentamicin (10) % Amikacin(30 ) % Imipenem(10 ) % 56
70 Clinical Isolates Fig 3 Bar Diagram of Antibiotic susceptibility pattern Sensitivity to Quinolones, Cotrimaxole, Nitrofurantoin and Gentamicin varied from 20% - 44%. Most of the species were highly sensitive to Amikacin and Imipenem, 83.3% and 87.8% respectively. 57
71 Antibiotic susceptibility pattern of various isolates: Antibiotic susceptibility test was done by disc diffusion method as per CLSI guidelines. The susceptibility of various isolates to the drugs is shown below. Name of GNB Table 9: Antibiotic susceptibility pattern of various isolates Ampi Cipro Genta Amikac Nitro Cotri Ceftazi Cefotax Ceftri Imp Amc E.coli 4 (3.8%) 22 (20.9%) 35 (33.3%) 93 (88.6%) 65 (61.9%) 20 (19%) 6 (5.7%) 10 (9.5%) 14 (13.3%) 94 ((89.5%) 10 (9.5%) Klebsiella 0 17 (33.3%) 24 (47%) 38 (74.5%) 13 (25.5%) 17 (33.3%) 6 (11.8%) 5 (9.8%) 10 (19.6%) 43 (84.3%) 2 (3.9%) Pseudomonas 0 25 (67.6%) 27 (72.9%) 34 (91.9%) 2 (5.4%) 3 (8.1%) 13 (35.1%) 11 (29.7%) 12 (32.4%) 30 (81%) 0 (%) Acinetobacter 0 2 (33.3%) 3 (50%) 4 (66.7%) 0 (%) 2 (33.3%) 0 1 (16.7%) 0 3 (50%) 0 (%) Enterobacter (%) 0 (%) Citrobacter 1 (33.3%) 0 (%) 2 (66.7%) 1 (33.3%) 2 (66.7%) 1 (33.3%) (100%) 1 (33.3%) 58
72 Ampi Cipro Genta Amik Nitro Cotri ceftazi Cefotax Ceftri Imp Amc E.coli Klebsiella Pseudomonas Acinetobacter Enterobacter Citrobacter Fig 4 Antibiotic susceptibility pattern of various isolates 59
73 Most of the species were resistant to Ampicillin. Among the E.coli (n =105) resistance to Ciprofloxacin was observed in 83 cases, Cotrimaxole resistance in 85 cases, Nitrofurantoin resistance in 40 cases, and resistance to and Amikacin was 11 and Imipenem was12 cases.. Of the 51 isolates of Klebsiella species included in the study resistance to Ciprofloxacin was observed in 34 cases, Cotrimaxole resistance in 34 cases, Nitrofurantoin resistance in 48 cases, and resistance to Imipenem and Amikacin was observed in 08 and 13cases respectively. Of the 37 isolates of Pseudomonas spp., 12 were resistance to Ciprofloxacin, 34 were Cotrimaxole resistance, resistance to Amikacin and Imipenem was 13 and 07 respectively ESBL production Combined disc test Table 10: ESBL production in clinical isolates GNB isolates Combined Disc Positive ESBL : Antibiotic susceptibility pattern to cefoxitin by disc diffusion: Amp C production (cefoxitin resistance) was tested by disc diffusion method according to CLSI guidelines. Strains exhibiting zone diameter 18mm were taken as resistant, 21 mm as sensitive and 18 21mm as intermediate sensitive. 60
74 Table 11: Antibiotic susceptibility pattern to cefoxitin No. of isolates Sensitive Intermediate Resistant : AMP C DISC TEST: The isolates that showed cefoxitin resistance was tested for Amp C Disc test, the results of which are shown in Table 15. Table :12: AmpC disk test results Total Indentation Flattening Negative isolates which showed resistance to cefoxitin was subjected to AmpC disc test, 50 of them showed indentation, and 20 showed flattening, while 5 isolates did not give positive results. The Amp C disk test is rapid, simple, convenient, and gives accurate results in detecting plasmid-mediated Amp C β lactamases. Cefoxitin resistance may be caused by Amp C production or non β lactamase mechanisms, such as reduced outer membrane permeability (porin mutations). The other mechanism such as (porin deficiency) may have contributed to the difference. 61
75 5.15: Antibiotic susceptibility pattern to Imipenem/Meropenem by disc diffusion: The sensitivity test was done by disc diffusion test. Isolates were considered sensitive if in the range of zone diameter 23 mm, resistant if zone diameter 19mm and intermediate if between 20-22mm diameter. Meropenem sensitivity was detected by disc diffusion method and MIC determination was done by Agar dilution technique. Isolates were considered sensitive if zone diameter was 23mm, intermediate sensitive if in range of mm, resistant if zone diameter was 19mm Table 13 A: Antibiotic susceptibility pattern to Imipenem (Disc diffusion) No. of isolates Sensitive Intermediate Resistant Table13 B: Antibiotic susceptibility pattern to Meropenem (Disc diffusion) No. of isolates Sensitive Intermediate Resistant
76 5.16: MBL detection by phenotypic methods: All the strains were subjected to MBL detection (n=204) by Modified Hodge test and Combined disc test. Isolates tested Imipenem resistant (n=25) Meropenem resistant (n=28) Table 14: Phenotypic detection of MBL Modified Hodge test Positive Combined disc test Positive Other isolates : Meropenem MIC by agar dilution method: All those strains which have MIC 1μg/ml are sensitive, 2-4μg /ml are intermediate strains and which have MIC range 4μg/ml are resistant. Table 15: Meropenem MIC Total isolates No. sensitive No. resistant No. intermediate MIC in μg/ml : Ceftazidime MIC by agar dilution method: The strains having MIC of 4μg/ml are sensitive, while the isolates in the range of 8 μg/ ml -16μg /ml are intermediate, and those strains which have MIC 16μg/ml are resistant. 63
77 Table 16: Ceftazidime MIC Total isolates No. sensitive No. resistant No. intermediate MIC in μg/ml Of the 204 isolates, 179 isolates had resistance to Ceftazidime, while 25 isolates were resistant to other third generation Cephalosporins (Cefotaxime, Ceftriaxone). 5.19: Detection of resistance genes by PCR: Table 17: Detection of resistance genes Organism No. tested TEM positive SHV positive IMP positive Escherichia coli Klebsiella spp Pseudomonas spp Randomly selected 10 study isolates were tested for resistance genes (TEM, SHV, IMP) by PCR. Out of 10, TEM and SHV genes were positive in all isolates, 2 isolates were positive for IMP gene. TEM, SHV gene were identified in Klebsiella pneumoniae, Escherichia coli and Pseudomonas species. IMP gene was detected in Klebsiella spp, and Pseudomonas spp. 64
78 5.20: Occurrence of beta lactamases: Beta lactamases occurred singly or in combinations which is illustrated in fig 5. Frequency of various enzymes ESBL,AmpC & MBL 10 ESBL & MBL AmpC & MBL 3 2 ESBL &AmpC 31 MBL 13 Number AmpC 27 ESBL Number of isolates 140 Fig 5: Occurrence of beta lactamases The beta lactamases occurred either singly or in combination.esbl was common beta lactamase produced. About 118 isolatess producedd ESBL alone, 27 isolates Amp C alone, 13 isolates MBL only. Combination of various enzymes was also noted. ESBL and Amp C found in 31 cases, ESBL and MBL in 3cases,Amp C and MBL in 2 cases, all three enzymes in 10 cases. Thus total ESBL production was in 162 cases, total Amp C production seen in 70 cases, and MBL in 28 cases. 65
79 5.21: Distribution of beta lactamases among isolates: Beta lactamase distributions among various isolates are shown in Table 18. Table 18: Beta lactamase distribution among various isolates Name of GNB No of isolates E. coli 105 Klebsiella 51 Pseudomonas 37 Acinetobacter 6 Enterobacter 2 Citrobacter 3 ESBL Amp C MBL Combinations 73 (61.9%) 22 (18.6%) 15 (12.7%) 3 (2.5%) 2 (1.7%) 3 (2.5%) 7 (25.9%) 11 (40.7%) 9 (33.3) - 5 (38.5%) 4 (30.8%) 1 (7.7%) 3 (23.1%) (43.47%) 14 (30.43%) 12 (20.08) Most of the E.coli isolates showed predominant production of ESBL while AmpC was common in Klebsiella spp, and Pseudomonas spp. 5.22: Distribution of beta lactamases among OPD and IPD AmpC and ESBL s were found in OP specimens also. Only 1 isolate showed resistance to all three enzymes. The distribution is shown below Table 19: Distribution of beta lactamases among OP and IP No.of isolates ESBL Amp C MBL Esbl& Amp C ESBL&MBL Amp C &MBL All three OP 17 (14.4%) 6 (22.2%) 1 (7.7%) 5 (16.1%) (10%) IP 101 (85.6%) %) 12 (92.3%) 26 (83.9%) 3 (100%) 2 9 (90%) 66
80 5.23: Distribution of ESBL Amp C and MBL in various specimens: The various samples showed the presence of single, or combination of enzyme production as shown in table below. Table 20: Distribution of ESBL Amp C and MBL in various specimens Organism No.of isolates ESBL AMP C MBL Combination Urine (62%) 11 (11%) 6 (6%) 21 (21%) Pus (51.7%) 08 (13.8%) 03 (5.2%) 17 (29.3%) Sputum (60.1%) 7 (23.3%) 1 (3.3%) 4 (13.3%) Swabs 09 5 (55.6%) 1 (11.1%) - 3 (33.3%) Catheter tip (66.7%) - 01 (33.3%) - Tracheal tip (100%) - Tissue (50%) - Blood 01 01(100%)








81 COLOUR PLATES COMBINED DISC TEST FOR ESBL CAZ CAC Ceftazidime CEFTAZIDIME AND CLAVULANIC ACID POSITIVE ZONE OF INHIBITION > 5mm



















82 AMP C DISC TEST A : PRESENCEE OF BLUNTING TOWARDS CEFOXITIN DISC. B&C : ABSENCE OF BLUNTING TOWARDS CEFOXITIN DISC.

















83 COMBINED DISC TEST POSTIVE : ZONE OF INHIBTION IS > 7MM BETWEEN IMIPENEM AND IMIPENEMM +EDTA
















84 MIC: MEROPENEM: AGAR DILUTION TECHNIQUE 4 gm Concentration 16 gm Concentrationn







85 32 gm Concentrationn CONCENTRATIONS OF ANTIBIOTIC WAS.5 ΜG TO 264ΜG PC : POSITIVE CONTROL NC : NEGATIVE CONTROL










86 MODIFIED HODGE TEST LAWN CULTURE OF E.coli ATCC25922 POSITIVE ENCHANCEMENT OF GROWTH AROUND IMIPENEM DISC.


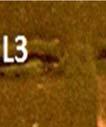



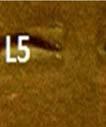





87 AGAROSE GEL ELECTROPHORESIS IMP GENE L1 NEGATIVE CONTROL L4M-100 bp molecular size standard DNA ladder( ,300,to 1000,1500) L2, L3 L5, L6, L7, L8 SAMPLES PRODUCT SIZE 220 bp POSITIVE L2 L3









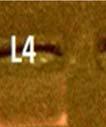
88 AGAROSE GEL ELECTROPHORESIS- TEM GENE L3 M-1000 bp molecular size standard DNA ladder ( ,300,to 1000,1500) L1NEGATIVE CONTROL L2, L4, L5, L6, L7, L8 SAMPLES PRODUCT SIZE262BP L2,L4,L5,,L6,L7,L8POSITIVE














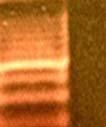
89 AGAROSE GEL ELECTROPHORESIS SHV GENE L2 M-1000 bp molecular size standard DNA ladder ( ,300,to 1000,1500) L1NEGATIVE CONTROL L3, L4, L5, L6, L7, L8 SAMPLES PRODUCT SIZE276bp L3, L4,L5, L6,L7,L8 POSITIVE
90 Discussion
91 6.DISCUSSION Antimicrobial resistance is a growing threat worldwide. Increasing resistance to third generation cephalosporins has become a cause for concern among Enterobacteriaceae. (55) The efficacy of beta lactam antibiotics has been reduced by production various types of beta lactamases. Beta lactamases have been characterized based on amino acid and nucleotide sequences. Four distinct classes are identified. Extended spectrum β lactamases belong to Class A, Metallo β lactamases Class B, Amp C β lactamases Class C and Cloxacillin hydrolysing β lactamases Class D (63) The indiscriminate use of the beta-lactam antibiotics offers selective pressures which lead to development of selected mutated forms of β-lactamases such as the ESBLs, AmpC β-lactamases and metallo-β-lactamases which have emerged as the most important resistance mechanism. This poses a therapeutic challenge to the health care settings. (47) Since Amp C production is accompanied by multidrug resistance, therapeutic options become limited and failure to identify them, results in inappropriate treatment. The occurrence of extended spectrum βlactamases (ESBLs) and AmpC among members of Enterobacteriaceae are common. Nowadays therapeutic failure is common among beta lactam antibiotics. (34) Metallobetalactamases is a group of carbapenem hydrolysing β lactamases. MBL are inhibited in vitro by chelating agents like EDTA, FeCl3, 68
92 2 mercaptoethanol and 2 mercaptopropionic acids. (63) Their detection is important as treatment options for them are very minimal, in such cases, usually Aztreonam, Polymyxin B or Colistin is used for treatment. The members of Enterobacteriaceae are the most frequent human pathogen in causing infections and isolated many a times from clinical samples. In the present study, a total of 204 isolates showing resistance to Ceftazidime, Cefotaxime or Ceftriaxone were selected from 492 GNB samples. These consisted of urine constituting 49.01% (100/204), pus 28.43% ((58/204) and sputum 14.7% (30/204) (Table: 2). Our study showed that among the isolates, E. Coli was predominant accounting to 51.47% (105/204) followed by Klebsiella spp about 25% (51/204), Pseudomonas spp % (37/204) Acinetobacter spp 2.94% (6/204) Citrobacter spp. 1.47% (3/204) and Enterobacter spp. 0.98% (2/204) (Table 4). This finding was on par with other studies by Metri et al (66) and Mathur et al, (44) where the E.coli was the predominant organism isolated. The antibiotic sensitivity pattern of beta lactamase producers revealed that maximum susceptibility was seen for Imipenem and Amikacin 87.8%, and 83.3% respectively. Sensitivity to Quinolones, Cotrimaxole, Gentamicin and Nitrofurantoin was 32.4%, 21.1%, 44.62%, and 40.2% respectively. Most of the isolates showed decreased susceptibility to Ampicillin and Amoxy clav drugs, 2.45% and 6.37% respectively.(table:8) 69
93 All the isolates that were showing resistance to one of the third generation Cephalosporins (Ceftazidime, Ceftriaxone and Cefotaxime) were taken for the study, as they are potential isolates showing either ESBL or AmpC β-lactamases or MBL production. In our present study, 492 gram negative clinical isolates were collected to study the prevalence of beta lactamases. Out of 492 isolates, 204 showed resistance to one or more of third generation cephalosporins. The prevalence of beta lactamases production was 204/ 492 isolates accounting for 41.4%. A study by Vijaya Doddaiaha et al accounts a prevalence of % (48) correlating to our study. In our study, expressions of various β-lactamases occurred, either singly ( ESBL, Amp C, MBL) or in combinations like ( ESBL +Amp C, ESBL + MBL, Amp C + MBL,ESBL +AMP C +MBL).The combination of ESBL/MBL/ AmpC β- lactamases was observed in 46 isolates 46 / 204. (Fig 5) Presence of multiple classes of β-lactamases in a single organism may pose a serious challenge in therapeutics. (38) It was found that the total ESBL producers were % (162/492). Among the 162 organisms producing ESBL, we found that 118 strains produced only ESBL (118/162), and further their combinations ( ESBL +AmpC ) were found in 31 strains (31/162 ),(ESBL +MBL)was in three strains ( 03/162), and ESBL with both AmpC and carbapenemase was in 10 strains ( 10/ 162). Fig 5 These results were comparable with the study from Karnataka by Vijay Doddehia et al where ESBL production was 34.04%. (48 ) 70
94 30.8% isolates were ESBL positive in a study by Rajesh Bareja in Haryana. (70) Babypadmini et al (45) studies on ESBL showed prevalence to be 40% which are comparable to our study. Similarly Rodrigues C. et al have evaluated 286 resistant isolates and reported 151 as ESBL producers, and with Amp C as 131/151, the combination which when compared to our study is high. (54) Co-existence of Extended spectrum β- lactamases and MBL were detected in 3/100 cases in a study by Malini et al (50). Two Indian studies Varsha et al and by Kumar et al showed prevalence of ESBL as 63.8 % (24) and 63.7% (46) respectively, and a study from. Devangree also shows high prevalence of 61.7% (57) which might be due to indiscriminate use of higher generation antibiotics. ESBL production was highest in E. coli (61.9%) isolates and followed by Klebsiella spp. 18.6%. Since the number of isolates of Enterobacter spp., Citrobacter spp. and Acinetobacter spp. are less, they are statistically not significant. (Table: 18) Detection rates across the country vary from 27.2% to 63.7% in E.coli for ESBL and 14% to 97.1% in Klebsiella spp. Sreekanth et al, report that among ESBL producers, 72.6% isolates of E. coli, and 22.6% isolates were Klebsiella spp. (65) correlating with our study. Rudresh et al from Bangalore too reported ESBL production is highest in E.coli about 65%. (59) 71
95 In Pseudomonas spp. ESBL production is12.7% which is lesser when compared to Enterobacteriaceae. This decreased incidence in Pseudomonas spp may be due other bacterial resistance mechanism such as the lack of drug penetration, the loss of certain outer membrane proteins and due to mutations in the porins and efflux pumps. (1) Amp C: In the present study, prevalence of Amp C was %. ( 70/492) (Table: 12) 27 isolates produced only Amp C, 31 isolates of AmpC coexisted with ESBL. 2 isolates of MBL coexisted with AmpC and all three enzymes occurred in 10 isolates. Rajesh Bareja et al study showed a prevalence of AmpC % (70) was similar as our study. A study from North India,at Guru Teg Bahadur Hospital by Vikas Manchanda, Delhi found AmpC enzyme producers among Gram negative bacteria was 20.7% (33) and another study from South India by Mathur et al reported 22.2% of AmpC producers both are concordant with our study. [44] Yet another study at Kolkatta showed prevalence of 6.7% which is less comparable with our results [53]. Another study also had low prevalence of Amp C production as 8%. [44] In contrast, studies from various other areas show high prevalence. A Study from South India by Anita Pandey et al showed highest prevalence of AmpC of 47%. [51] Amp C production was predominant in Klebsiella spp, (34.8%) followed by E.coli (19.45%) in our study. 72
96 The only drug of choice in ESBL and Amp C resistant isolates was carbapenems, but due to their irrational use the carbapenem resistance is increasing and mostly due to MBL production. (56) It has been reported that some MBL producing GNB are difficult to detect because they are inhibited by low concentrations of IMP, thus they might give false susceptibility result by disc diffusion. So testing of all Cephalosporin resistant strains was recommended for detection.hence we subjected all the strains that were resistant to third generation cephalosporin for confirmatory test for carbapenamases. Most isolates were susceptible to Imipenem except 25 isolates (25/204). Resistance to Meropenem was also detected and it was found in 28 isolates (28/204). (Table13) Except 3, all isolates which showed resistance to Meropenem were also resistant to Imipenem. This was confirmed by MIC, where 28 isolates showed MIC >2μg. (Table: 15)In the current study, we majority of the isolates were sensitive to Imipenem, which was concordant with other studies. Similar findings were seen in another study from Coimbatore. (58) In the current study production of MBL was seen in 5.69 %( 28/492). (Table 13) A study from North India (Priya dutta et al) shows MBL production to be 7.86%. (68) They attribute this low prevalence of MBL to stringent antibiotic stewardship program Another study by Nagdeo et al also showed the prevalence of MBL as 7.44%. (6) Results of both studies are similar to our study. 73
97 A surveillance study by Wattal C et al in New Delhi reports a high prevalence of resistance to Imipenem & Meropenem as 2 and 13% in E. coli and in Klebsiella spp.as31&51%. (62) High prevalence of resistance varying from 17% to 22%was reported by Gupta E et al. among Enterobacteriaceae strains. (61) Production of high prevalence of MBL was reported from a study by Kalpana Chauhan in Meerut. [51] and Malini et al (50) as 20.6% and 30% respectively. The prevalence is low in our study. It may be due to using Carbapenem as a reserve drug for the treatment of multidrug-resistant Gram-negative pathogens only. The production of all three enzymes (ESBL +Amp C +MBL) was 2.03% (10/492) (Fig :5) All three enzymes were simultaneously detected in (4.21%) of cases in a study by Nagdeo et al which very well correlates with our study, (6) The distribution of the three enzyme classes among all the species shows a characteristic pattern. When resistance was conferred by producing a single enzyme, it was commonly the ESBL producer but AmpC and MBLs were more commonly seen when the multiple enzyme production was observed. In this study, 2.03% of the total isolates produced all the three, viz, ESBL, AmpC, and MBL. Although, prima facie the number appears to be small, it sounds an alarm for existence of highly resistant pathogens. 74
98 This study results indicate that ESBL production is a major mechanism of resistance to cephalosporins among Gram-negative bacteria. Our study of phenotypes indicative that Enterobacteriaceae produce ESBL, AmpC, and MBL, but with varying frequencies. Over three fourth of strains produce ESBL s; one third of them produce AmpC and about a minimal number of strains produced MBL. While most of the Gram-negative organisms tend to produce ESBL more frequently, Klebsiella spp produces AmpC, and nonfermenters tend to produce AmpC and MBLs. Beta lactamases producing isolates, in addition to being resistant to ß lactam antibiotics, are also resistance to other classes of drugs like Tetracycline Gentamicin, Cotrimoxazole, and Fluoroquinolone. (55) Multiple drug resistance (resistance to three or more drugs ) and resistance to five or more drugs were also observed. In our study also we observed that the ESBL and MBL producing isolates were often resistant to other classes of drugs like quinolones and Aminoglycosides. (Table: 8) This could be due to co-existence of genes encoding drug resistance to those antibiotics on the plasmids carrying ESBL and MBL. Treatment options for carbapenem resistant strains of Enterobacteriaceae are limited. Current treatment for these infections is Colistin, Fosfomycin, Tigecycline and Temocillin. 75
99 Considering PCR as the gold standard, we selected few strains to detect the genes for ESBL and MBL. All the ten isolates selected showed the presence of TEM and SHV genes, and 2 isolate showed the presence of IMP gene. (Table 17) The strains which were negative for IMP gene could harbor other carbapenamase genes. The study underlines the problem of ESBL, AmpC and MBL mediated resistance, which has created a therapeutic challenge for the clinicians and microbiologists. Simple disc method can be routinely employed to detect these common resistance mechanisms, which will reduce the mortality and spread of these resistant strains. Thus the rapid and convenient phenotypic screening tests can be used to detect them in the clinical laboratory. 76
100 Summary
101 7. SUMMARY 1. Gram negative bacilli which are beta lactamases producers have become the important emerging pathogens. 2. The members of Enterobacteriaceae are the most frequent human pathogen in causing infections and are isolated mostly from clinical samples. Due to increased production of beta lactamases (ESBL, Amp C s or MBL) among these pathogens, the treatment becomes difficult in these infections. 3. The antibiotic susceptibility profile of our study revealed that susceptibility of beta lactamase producers to Imipenem and Amikacin were found to be 87.8%, and 83.3% respectively. Sensitivity to Quinolones, Cotrimaxole, Gentamicin and Nitrofurantoin were 32.4%, 21.1%, 44.62%, and 40.2% respectively. Majority of the isolates found to have decreased susceptibility to Ampicillin and Amoxy clav drugs. (2.45% and 6.37%) 4. The prevalence of beta lactamase production in GNB in our study was found to be 41.4%. 5. Total ESBL producer was32.94%. The occurrence of beta lactamases producers in various isolates in this study showed, that E.coli was the common ESBL producer. 6. Total Amp C production was14.22%. The major Amp c producer was Klebsiella species. 77
102 7. Total MBL production was 5.48%, which is very low when compared to other similar studies. 8. It was observed in our study that ESBL co existed with Amp C and MBL, and it was also found that Amp C also coexisted with MBL. The co production of the ESBL + MBL + AmpC β- lactamases was also observed. 9. The distribution of the combinations was as follows, 118 strains produced only ESBL (118/162). The combinations like ( ESBL +AmpC ) were found in 31 strains (31/162 ),(ESBL +MBL)was found in three strains (03/162), and ESBL with AmpC and carbapenemase was seen in 10 strains ( 10/ 162). Similarly Amp C coexisted with MBL in 2 strains. 10. ESBL production coexisted with resistance to several other antibiotics.in our study, the resistance to third generation Cephalosporins was found to coexist with resistance to other antibiotics like Ampicillin, Cotrimoxazole, Nitrofurantoin and Ciprofloxacin. 11. Occurrence of multi-drug resistance to the third generation cephalosporins, Aminoglycosides and Fluoroquinolone is common among beta lactamase producers., our observation is that beta lactamase producing isolates were significantly more resistant to Ampicillin (97.55%), Amoxy clav (93.63%), Cotrimoxazole (78.9%), Nitrofurantoin (59.8%), Ciprofloxacin (67.6% ) and Gentamicin ( 55.38%). 78
103 Conclusion
104 8. CONCLUSION The study conducted in our hospital highlights the emerging prevalence of beta lactamases. The consequences of antibiotic resistance lead to longer duration of illness, treatment with expensive drugs, higher mortality and increased burden on the health system. Since carbapenamase enzymes have the potential of easy transmission via transposons and/ or integrons, there is a high chance to disseminate among susceptible gram negative bacterial isolates in the hospital. Hence reporting of beta lactamases production along with routine antibiotic susceptibility testing should be done in every lab, in order to guide the physicians to choose the appropriate antibiotics. We must have a functional hospital infection control committee with appropriate antibiotic policy and regular updates, to prevent the spread of, Amp C, ESBL and MBL. Each and every antibiotic usage in hospital should be documented which will help us to develop dosing strategies. In order to select of appropriate therapeutic schemes, additionally detection and surveillance of beta lactamases production becomes a matter of major importance for the implementation of infection control measures. All attempts should be made to prevent dissemination of beta lactamases in the community. One should keep Carbapenems as a reserve drug, and should be used only for multidrug resistant bacteria. 79
105 Annexures
106 ANNEXURE I Functional and Molecular classification schemes for bacterial β-lactamases Function Class Molecular Class Preferred substrate Inhibited by Ca EDTA 1 C Cephalosporins - - Representative Enzymes Amp c enzymes GNB 2a A Penicillins + - Pencillanases GPB 2b 2be A A Penicillin, Cephalosporin Penicillin, ESBL, Monobactams br A Penicillin +/- - 2c 2d A D Penicillin, Carbenicillin Penicillin, Cloxacillin + - +/- - 2e A Cephalosporin + - 2f A 3 B Penicillin, Cephalosporins, Carbapenems Most β-lactams including Carbapenems +/ ND Penicillin -? TEM1, TEM 2, SHV1 TEM3-26, SHV2-6, Klebsiella oxytoca TEM 30-36, TRC-1 PSE 1, PSE 3,4 OXA 1-11, PSE 2 Inducible Cephalosporinases from P. Vulgaris NMC from Enterobacter sp Sme-1 from Serratia marcescens L1 from Xanthomona smaltophila,ccr A Bacteroides fragilis Penicillinase from Pseudomonas cepacia
107 ANNEXURE II PCR Procedure: 1. Overnight culture centrifuged at 6000rpm for 5min 2. Supernatant discards and the Pellet is suspended in 200µl of PBS. 3. Added 20µl of Lysozyme and 180ul of Lysozyme digestion buffer mixed. 4. Incubated at 37ºC for 15min µl of Binding buffer and 20µl of Proteinase K [10mg/ml] is added and gently mixed well. 6. Incubated in water bath at 56 C for 10 min ul of Isopropanol mixed. 8. Transferred whole lysate into Pure Fast spin column and centrifuged at 10000rpm for 1min. 9. Discard flow through and added 500µl of Wash Buffer-1 and Centrifuge at 12000rpm 1 min. 10. Discard flow through and added 500µl of Wash Buffer-2 and centrifuged at 12000rpm for 1min. Repeated wash one more time. 11. Discarded flow through and Centrifuged column for additional 2 minute to remove any residual ethanol. 12. Eluted DNA by adding 100µl of Elution Buffer and Centrifuged for 1min. 13. Quality and Quantity of extracted DNA is checked by loading in 1% agarose gel and 5µl of extracted DNA is used. Primers used: HELINI TEM gene primer Forward Primer: 5'-GATAACACTGCGGCCAACTT -3' Reverse Primer: 5'-CTGCAACTTTATCCGCCTCC PCR-3' Product size: 262bp HELINI -SHV gene primer Forward Primer: 5'-CGCCGCCATTACCATGAGCGAT -3' Reverse Primer: 5'-ACCCGATCGTCCACCATCCACT PCR-3' Product size: 276bp HELINI -IMP gene primer Forward Primer-5'-TTTTGCAGCATTGCTACCGC-3' Reverse primer-5'-cacgctccacaaaccaagtg-3' Product size = 220bp
108 PCR Procedure: [25µl of Master Mix contains: 10X Taq buffer, 2mM Mgcl2, 0.4mM dntps mix, and 2U Taq DNA polymerase] 1. Reactions set up as follows; Components In PCR vial Master mix. Reactions set up as follows; Components In PCR vial Master mix Quantity 10µl Quantity 10µl Primer - forward(2pmoles/µl) 5µl Primer- reverse(2pmoles/µl) 5µl Genomic DNA 5µl Total volume 25µl 2. Mixed gently and spin down briefly. 3. Place into PCR machine and program it as follows; Initial Denaturation: 94ºC for 3 min Denaturation: 94ºC for 1 min Annealing: 58ºC for 1min 35 cycles Extension: 72ºC for 1min Final extension: 72º C for 5 min Gel electrophoresis: Prepare 2% agarose gel. [2gm of agarose in 100ml of 1x TAE buffer] 2. Mix 8µl 6X Gel loading dye to each PCR vial and loaded entire PCR product. 3. Run electrophoresis at 50V till the dye reaches three fourth distances and observe the bands in UV Transilluminator.
109 ANNEXURE III SCHEME FOR PREPARING DILUTIONS OF ANTIMICROBIAL AGENTS TO BE USED IN AGAR DILUTION SUSCEPTIBILTY TESTS STEPS CONC(Μg/ml) source Volume Diluents Immediate conc. Final conc. At1:10 dilution 5120 stock stock stock stock Step Step Step Step Step Step Step Step Step
110 ANNEXURE IV LIST OF TABLES S. No. TOPICS 1. DISTRIBUTION OF ISOLATES 2. DISTRIBUTION OF ISOLATES IN SAMPLES 3. SAMPLES COLLECTED WARDWISE 4. DISTRIBUTION OF SAMPLES IN VARIOUS WARDS 5. No. OF GNB ISOLATED 6. DISTRIBUTION OF ISOLATES IN VARIOUS WARDS 7. CLINICAL SPECIMEN AND ORGANISM ISOLATED 8. ANTIBIOTIC SUSCEPTIBILTY PATTERN 9. ANTIBIOTIC SUSCEPTIBILITY PATTERN OF VARIOUS ISOLATES 10 ESBL PRODUCTION IN CLINICAL ISOLATES 11. ANTIBIOTIC SUSCEPTIBILITY PATTERN TO CEFOXITIN 12. AMP C DISK TEST 13.A ANTIBIOTIC SUSCEPTIBILITY PATTERN TO IMIPENEM 13.B ANTIBIOTIC SUSCEPTIBILITY PATTERN TO MEROPENEM 14. PHENOTYPIC DETECTION OF MBL 15. MEROPENEM MIC 16. CEFTAZIDIME MIC 17. DETECTION OF RESISTANCE GENES 18. BETA LACTAMASE DISTRIBUTION AMONG VARIOUS ISOLATES 19. DISTRIBUTION OF BETA LACTAMASE AMONG OP AND IP 20. DISTRIBUTION OF ESBL AMP C AND MBL IN VARIOUS SPECIMENS
111 ANNEXURE V LIST OF GRAPHS 1. AGEWISE DISTRIBUTION OF ISOLATES 2. SEX WISE DISTRIBUTION OF ISOLATES 3. BAR DIAGRAM OF ANTIBIOTIC SUSCEPTLBILTY PATTERN 4. ANTIBIOTIC SUSCEPTLBILTY PATTERN OF VARIOUS ISOLATES 5. OCCURENCE OF BETA LACTAMASES
112 ANNEXURE VI LIST OF ABBREVIATIONS GNB CLSI ESBL MBL PBP MHA ATCC MIC PCR RFLP DDST CDT IPM CAZ CTX EDTA OPD IPD ICU MSW MMW FMW FSW ENT HVS 3GC GRAM NEGATIVE BACTERIA CLINICAL AND LABORATORY STANDARDS INSTITUTE EXTENDED SPECTRUM BETA LACTAMASES METALLO BETA LACTAMASES PENCILLIN BINDING PROTEINS MULLER HINTON AGAR AMERICAN TYPE CULTURE COLLECTION MINIMUM INHIBITORY CONCENTRATION POLYMERASE CHAIN REACTION RESTRICTION FRAGMENT LENGTH POLYMORPHISM DOUBLE DISC SYNERGY TEST COMBINED DISC TEST IMIPENEM CEFTAIDIME CEFOTAXIME ETHYLENE DIAMINE TETRA ACETIC ACID OUTPATIENT DEPARTMENT INPATIENT DEPARTMENT INTENSIVE CARE UNIT MALE SURGICAL WARD MALE MEDICAL WARD FEMALE MEDICAL WARD FEMALE SURGICAL WARD EAR NOSE &THROAT HIGH VAGINAL SWAB 3 RD GENERATION CEPHALOSPORIN
113 KEY TO MASTER CHART ENZYME PRODUCTION 0 - PRESENCE OF THAT PARTICULAR ENZYME. ANTIBIOTIC SUSCEPTIBILITY 1 - SUSCEPTIBILE TO THAT ANTIBIOTIC. ESBL - MBL - EXTENDED SPECTRUM BETA LACTAMASES METALLOBETA LACTAMASES.
114 MASTER CHART S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 1 msw 50 m Wound swab E.coli msw 73 m Pus E.coli ent 34 m aural swab Pseudomonas paediatric 12 m Urine E.coli Gynaec 39 f Urine E.coli msw 74 m Tissue psedomonas msw 65 m Pus E.coli Gynaec 39 f Pus Klebsiella gynaec 65 f Urine E.coli Gynaec 65 f Pus Pseudomonas msw 26 m Urine E.coli Gynaec 35 f Urine Klebsiella fmw 23 f Urine E.coli icu 70 m sputum Klebsiella mmw 48 m urine E.coli fmw 48 f urine E.coli msw 70 m pus Citrobacter Gynaec 37 f urine e.coli Gynaec 60 f urine E.coli Gynaec 40 f urine E.coli icu 36 m sputum Klebsiella mmw 45 m urine Pseudomonas Gynaec 22 f urine E.coli icu 55 f urine E.coli o Gynaec 23 f pus E.coli msw 52 m urine Klebsiella
115 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 27 mmw 45 m urine Citrobacter Gynaec 30 f urine E.coli Gynaec 50 f HVS E.coli fmw 18 f urine E.coli Gynaec 31 f HVS Klebsiella msw 45 m pus Klebsiella msw 60 m pus E.coli op 35 f urine Klebsiella op 47 f urine E.coli fsw 48 f urine Klebsiella msw 65 m pus E.coli icu 26 f urine E.coli paediatric 3 f urine E.coli MSW 60 m pus E.coli fsw 40 f pus Pseudomonas icu 80 m urine E.coli msw 47 m pus E.coli mmw 35 m urine E.coli op 80 f urine E.coli op 39 f urine E.coli msw 75 m pus Pseudomonas fsw 40 f pus Klebsiella op 43 f urine Pseudomonas op 55 m urine E.coli Gynaec 47 f urine E.coli msw 40 m pus E,coli op 55 m sputum Klebsiella icu 45 m sputum Klebsiella
116 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 55 OP 60 f urine E.coli msw 75 m pus Klebsiella paediatric 3 m urine E.coli FSW 70 f pus Klebsiella gynaec 46 f pus Klebsiella MSW 42 m pus E.coli icu 77 m pus E.coli paediatric 12 f urine E,coli msw 57 M sputum Acinetobacter msw 60 m pus Klebsiella op 34 f urine E.coli op 57 m sputum Acinetobacter op 48 f urine e.coli icu 44 m pus Klebsiella fmw 45 f urine Klebsiella FMW 33 f sputum Pseudomonas Gynaec 39 f catheter tip E.coli op 33 f urine E.coli Gynaec 36 f urine Klebsiella fsw 45 f pus E.coli fmw 53 f urine E.coli icu 85 m urine Pseudomonas Fmw 15 f urine E.coli icu 55 f pus E.coli op 23 f urine E.coli mmw 27 m blood E.coli msw 48 m pus Klebsiella msw 19 f pus Klebsiella
117 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 83 ICU 50 f pus E.coli icu 25 f urine Klebsiella msw 38 m pus E.coli op 43 f urine E.coli op 52 m urine E.coli Gynaec 60 F urine E.coli Gynaec 43 f cervical swab Pseudomonas fmw 56 f urine E.coli Gynaec 48 f urine Pseudomonas icu 70 f pus Klebsiella msw 80 m urine E.coli op 24 f urine E.coli icu 41 f urine E.coli msw 56 m pus E.coli fsw 22 F pus E.coli op 41 m sputum Klebsiella icu 36 m sputum Pseudomonas icu 70 f pus Klebsiella icu 45 m pus Pseudomonas op 28 f urine Klebsiella icu 55 m urine E.coli gynaec 80 f urine Klebsiella mmw 50 m sputum Pseudomonas gynaec 50 f urine Pseudomonas mmw 20 m sputum Pseudomonas icu 25 m sputum Pseudomonas op 18 f pus Pseudomonas fsw 21 f sputum Pseudomonas
118 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 111 op 67 m urine E.coli fsw 25 f urine E.coli Gynaec 45 f urine E.coli op 46 f urine Klebsiella mmw 61 f urine Pseudomonas icu 38 f urine E,coli icu 54 m pus Klebsiella msw 45 m pus Acinetobacter fmw 62 f urine E.coli MMW 26 m sputum Pseudomonas ICU 55 f urine E.coli OP 22 f urine E.coli icu 62 m urine E.coli icu 60 m pus E.coli fsw 58 f pus Pseudomonas icu 30 f urine E.coli ICU 21 F sputum Klebsiella Gynaec 55 f urine E.coli fsw 55 f pus E.coli op 47 m sputum Pseudomonas paediatric 3 f urine E.coli ICu 67 m sputum Klebsiella ICU 80 m urine Pseudomonas op 35 f urine Klebsiella msw 60 m urine E.coli Gynaec 39 f sputum Pseudomonas fsw 50 f pus Pseudomonas mmw 30 m urine E.coli
119 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 139 ICU 60 m sputum Pseudomonas fsw 50 f pus Pseudomonas ICU 31 m trachel tip Klebsiella I ICU 12 m urine E.coli FSW 50 f pus Pseudomonas fsw 55 f urine E.coli MMW 20 m sputum Klebsiella OP 70 m sputum E.coli gynaec 50 f catheter tip Pseudomonas icu 41 m urine E.coli icu 25 m sputum Pseudomonas msw 45 m pus Klebsiella fmw 28 f urine E.coli icu 65 f pus Klebsiella icu 68 m sputum E.coli fmw 55 f urine E.coli op 47 f urine E.coli op 20 f urine E.coli msw 50 m pus E.coli icu 80 m pus E.coli mmw 55 m sputum Klebsiella icu 65 m urine E.coli gynaec 25 f urine E.coli fmw 45 f sputum Pseudomonas icu 30 f urine E.coli gynaec 40 f urine Klebsiella o msw 80 m pus Pseudomonas
120 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 166 icu 74 m sputum Klebiella msw 49 m pus Pseudomonas fmw 60 f urine E.coli icu 67 m urine E.coli op 30 f cervical swab E.coli mmw 60 m sputum Pseudomonas icu 58 m 173 icu 80 m wound swab wound swab E.coli Klebsiella fsw 27 f urine E.coli msw 38 m pus E.coli msw 30 m pus Enterobacter icu 16 m urine E.coli mmw 55 m urine E.coli fsw 35 f pus Acinetobacter paediatric 3 m urine E.coli fmw 76 f urine E.coli msw 49 m pus Klebsiella op 46 m urine Enterobacter msw 49 m pus Klebsiella mmw 52 m sputum Klesiella fmw 23 f urine Klebsiella msw 47 m urine Klebsiella o Gynaec 30 f urine E.coli msw 66 m sputum Klebsiella fsw 50 f pus Klebsiella icu 57 f tissue Klebsiela msw 43 m pus Klebsiella
121 S. No P. Status Age Sex Sample Organism ESBL AMP C MBL AMP I CIPRO Genta Ami kacin Nitrofur antoin Cotr Cefta zidime Cefo taxim Ceftri axone AMC Imi penem Mer penem 193 mmw 68 m sputum Pseudomonas gynaec 41 f woundsw ab Klebsiela Fsw 50 f pus Pseudomonas mmw 52 f urine E.coli gynaec 55 f urine E.coli mmw 40 m urine E.coli msw 46 m catheter tip Acinetobacter op 19 m urine E.coli mmw 35 m urine E.coli msw 45 m pus Klebsiella fmw 36 f urine citrobacter gynaec 28 f pus acinetobacter 0 1





122