Accepted Manuscript. Tag, You re It! Finding and Treating Early Lung Cancers in a Single Setting. Ngoc-Quynh Chu, MD, Yolonda L.
|
|
|
- Duane Lewis
- 5 years ago
- Views:
Transcription

1 Accepted Manuscript Tag, You re It! Finding and Treating Early Lung Cancers in a Single Setting Ngoc-Quynh Chu, MD, Yolonda L. Colson, MD, PhD PII: S (18) DOI: Reference: YMTC To appear in: The Journal of Thoracic and Cardiovascular Surgery Received Date: 19 December 2018 Accepted Date: 19 December 2018 Please cite this article as: Chu N-Q, Colson YL, Tag, You re It! Finding and Treating Early Lung Cancers in a Single Setting, The Journal of Thoracic and Cardiovascular Surgery (2019), doi: doi.org/ /j.jtcvs This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
2 Tag, You re It! Finding and Treating Early Lung Cancers in a Single Setting Ngoc-Quynh Chu, MD and Yolonda L. Colson MD, PhD Division of Thoracic Surgery, Department of Surgery, Brigham and Women s Hospital Conflict of Interest Statement: The authors have no connection to the published work. Stryker (Novadaq Industries) has provided an equipment loan for independent studies, and a sponsored research agreement with Canon USA is for an unrelated project (YLC). Corresponding author: Yolonda L. Colson MD PhD Division of Thoracic Surgery, Brigham and Women s Hospital 75 Francis Street Boston, Massachusetts Tel: (617) , Fax: (617) ycolson@partners.org
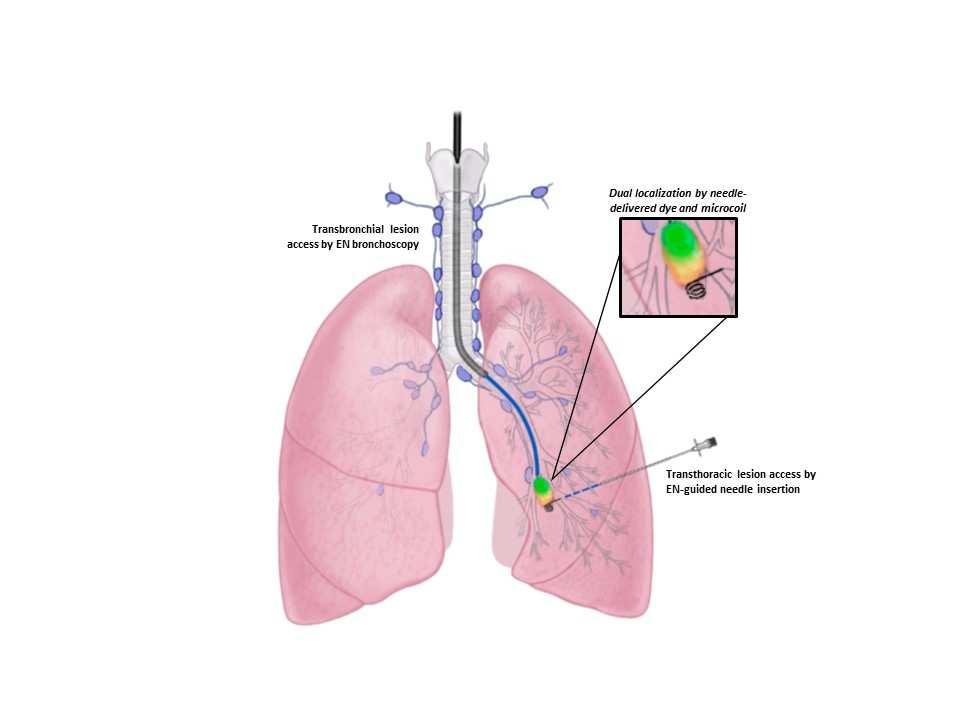
3 Manuscript: The increasing use of CT imaging and the advent of lung cancer screening has allowed for detection of potential cancers in the very early stages of disease. However, the size and characteristics of these radiologically visible pulmonary nodules (particularly ground glass opacities ) are often neither visible nor palpable in the operating room, making accurate tissue sampling and diagnosis uncertain and resection difficult. This challenge makes pre-operative lesion localization crucial and involves image guidance with CT or electromagnetic navigation (EN) bronchoscopy in conjunction with labeling by physical markers (hookwires, microcoils, fiducials) or dyes (patent blue, ICG). Additional intra-operative localization methods to confirm accurate localization are often needed as well (fluoroscopy, ultrasound, near-infrared imaging). 1 Hsu and colleagues describe a method for lesion localization that uses an EN-guidance system for percutaneous microcoil placement to mark a nodule for immediate thoracoscopic biopsy. Unlike preceding EN systems, the described technology allows for both bronchoscopic and transthoracic-guided routes of lung access. The investigators leverage the transthoracic capability to navigate to the lesion and deploy a microcoil through the biopsy needle to mark the target lesion. In the majority of the cases presented, a dye was also administered with the microcoil for dual localization. Immediate VATS biopsy was done, with additional intraoperative imaging to confirm marker location, prior to resection. In all cases, both the microcoil and the lesion of interest were within the resected specimen with a mean microcoil-to-lesion distance of 4.2 mm. Numerous groups have reported EN bronchoscopy (ENB) for the purposes of pleural dye marking of lesions for surgical resection, tissue collection for molecular profiling, fiducial marker placement to guide stereotactic body radiation therapy, and ICG-NIRguided mediastinal lymph node sampling. 2 The application of EN guidance for microcoil placement as reported here promises multiple benefits and is an innovative use of existing technology. Currently, microcoils are placed percutaneously under CT guidance to mark
4 the tumor site before the patient is transported to the OR for resection. The novelty in this report lies in percutaneous microcoil placement by EN guidance in the operative suite, allowing for immediate VATS resection. A major advantage of this approach is the streamlined workflow and condensed procedure time with microcoil placement and VATS biopsy performed during the same procedure, in the same room, and by the same team. This minimizes radiation exposure, likelihood of microcoil displacement (a not infrequent complication), and potentially hospital costs while rendering irrelevant the usual concern for pneumothorax after transthoracic biopsy or coil placement in the radiology suite. The addition of transthoracic capabilities to an ENB system is a useful feature, providing an additional means for biopsy, particularly when the diagnostic yield of transbronchial ENB remains generally lower than that of transthoracic needle biopsy. 2 While the number of patients reported in this study is small, safety and feasibility of what will become an increasingly common approach to identify and resect small nodules in the lung is demonstrated and will be a valuable technique in the treatment of early stage lung cancers at a size not previously possible. References: 1. Lin MW, Chen JS. Image-guided techniques for localizing pulmonary nodules in thoracoscopic surgery. J Thorac Disease (8, Suppl 9): S749-S Mehta AC, Hood KL, Schwarz Y et al. The evolutional history of electromagnetic navigation bronchoscopy. Chest (154):
5