The value of Immunogenecity. Gloria Vásquez Professor
|
|
|
- Merry Ross
- 5 years ago
- Views:
Transcription

1 The value of Immunogenecity Gloria Vásquez Professor
2 Conflictos de interés en los últimos 5 años He participado en actividades académicas y asesorías: Abbvie, Pfizer, BMS, Novartis, Glaxo, y Roche He recibido financiación para asistir a eventos académicos: Pfizer, Abbvie, Novartis He recibido información: Abbvie, Pfizer, Roche, BMS, Janssen, Lilly, Romers. La participación en este evento y el contenido de esta charla no tienen ningún fin comercial, ni ha sido influenciada por intereses económicos
3 Immunogenecity Definition Is the capacity of any molecule to induce a specific immune response, cellular or humoral, as a resulted to structural differences of exogenous molecules
4 What are the anti drug antibodies (ADAs)? Antibodies against proteins like therapeutic antibodies, fusion proteins or endogenous proteins. The ADAs against idiotypes could bind the variable region of antibodies in the place of antigen binding (neutralizing) or bind other domains of the antibodies (no neutralizing) Idiotype Drug Allotype Drug ADAs ADAs Valor L, de la Torre I.Reumatol Clin 2013;9:1-4

5 Anti drug antibodies
6 Arguments to demonstrate their importance Humanization of therapies Explanation of secondary failures Choice of therapy after 2 failure Demonstration of biosimilarity Continuous improvement
7 Inmunogenecity




8 Structural Aspects Determinants Structural properties of a protein Human Sequence Variation 2 A L C N A T F K K T K A L S N K A I F K K F Bacterial Post-translational Modifications 4 * Signaling Increased activity or serum half-life Monoclonal Antibody Type 2,3 O-glycosylation N-glycosylation Protein Folding 1 Murine Chimeric Humanized Human Phosphorylation Lipid attachment Omab Ximab Zumab Umab Activation or inhibition Cleavage Activation Membrane localization Glycosylation 2 * Immunogenicity *Not all biologics are glycoproteins glycosylation will not be relevant to all biologics 1. UMass. Workshops, Short Courses and Seminars Schellekens H. Nat Rev Drug Discov 2002;1:457 62; 3. Schellekens H. Clin Ther 2002;24: ; 4. Kuhlmann M, et al. Nephrol Dial Transplant 2006;21:4 8 8


9 Challenge reduce immunogenicity

10
11 Arguments to demonstrate their importance Humanization of therapies Explanation of secondary failures Choice of therapy after failure 2 Demonstration of biosimilarity Continuous improvement


12 Why a secondary failure? Wolbink GJ, et al. Arthritis Rheum Mar;54(3):711-5.

13 Plasencia,C et al. Ann Rheum Dis. 2012, 71:
14 Plasencia,C et al. Ann Rheum Dis. 2012, 71:

15 Anti-Drugs Antibodies and Drug Levels Carroscosa JM. Actas Dermosifilogr. 2013;104(6):
16 Adalimumab ADAs and treatment failure Bartelds GM et al. JAMA Apr 13;305(14):
17 Niveles valle de infliximab (μg/ml) ADAs may produce lower serum levels of the drug Median serum IFX levels (p=0,003) Positive (n=30) Negative/ indeterminate (n=20) Haraoui B, et al. J Rheumatol 2006; 33:31 36.
18 Arguments to demonstrate their importance Humanization of therapies Explanation of secondary failures Choice of therapy after 2 failure Demonstration of biosimilarity Continuous improvement

19 Secondary failure what to do? Vincent FB, et al Ann Rheum Dis Feb;72(2):165-78

20 The presence of antibodies and the choice of a new biological Antibodies are molecule-specific Jamnitski A, et al. Ann Rheum Dis Feb;70(2):284-8.
21 Proposal of a biological management algorithm 21

22 Differences in immunogenicity Moots RJ et al. PLoS One Apr 27;12(4):e


23 Differences in immunogenicity between TNF inhibitors There are differences in ADA frequency The frequency of ADA may be associated with a lower frequency of remission Moots RJ et al. PLoS One Apr 27;12(4):e
24 Anti-abatacept antibodies Nash P, et al. Arthritis Care Res (Hoboken) Oct 24. [Epub ahead of print
:1078-1085")
25 anti-tocilizumab antibodies Burmester GR. Ann Rheum Dis Jun;76(6):
26 Arguments to demonstrate their importance Humanization of therapies Explanation of secondary failures Choice of therapy after 2 failure Demonstration of biosimilarity Continuous improvement
27 WHO, EMA and FDA guidelines on immunogenicity and biosimilarity WHO Guidance 1,2 EMA Guidance 3,4 FDA Guidance 5 Immunogenicity should always be investigated in humans pre-authorization Biosimilar and reference product should be compared for frequency and type of ADAbs Potential consequences of ADAb development should be considered Immunogenicity data obtained during comparative efficacy trials usually will be sufficient Comparative evaluation of immunogenicity is important due to its potential clinical consequences Clinical significance of ADAb development may require investigation Additional investigation may be warranted if equivalence has been demonstrated through PD data or the biosimilar is from a different expression system Dose is an important consideration Demonstrating there are no meaningful differences in immune response is key to demonstrating biosimilarity Immune response criteria should be identified prospectively Extent and timing of assessment will depend on extent of similarity and incidence and clinical consequences of immunogenic reaction Minimum follow-up for chronically administered agents is 1 year ADAbs, anti-drug antibodies; EMA, European Medicines Agency; FDA, US Food and Drug Administration; PD, pharmacodynamic; WHO, World Health Organization. 1. WHO Guidelines on Evaluation of Similar Biotherapeutic Products. Geneva, Oct, 2009, 2. WHO Guidelines on the quality, safety, and efficacy of biotherapeutic protein products prepared by recombinant DNA technology, 2013, 3. EMA Guideline on similar biological medicinal products containing monoclonal antibodies non-clinical and clinical issues, May 2012; 4. EMA CHMP Guideline on immunogenicity assessment of monoclonal antibodies intended for in vivo clinical use, Dec 2012; 5. FDA Guidance for Industry. Scientific Considerations in Demonstrating Biosimilarity to a Reference Product. HHS FDA/CDER/CBER, Apr
28 Ann Rheum Dis Oct;72(10): Keiserman M et al. Expert Rev Clin Immunol Aug;10(8):
:1613-20 Keiserman M et al.")
29 Ann Rheum Dis Oct;72(10): Keiserman M et al. Expert Rev Clin Immunol Aug;10(8):
30
31 Differences in Comparative Immunogenicity: EMA and FDA Guidance EMA Guidance 1 Higher immunogenicity in the biosimilar: May be an issue for benefit/risk analysis May question degree of biosimilarity Lower immunogenicity in the biosimilar: Would not preclude biosimilarity Additional safety/efficacy analyses should be conducted on patients who did not develop ADAbs FDA Guidance 2 Differences in immune response in the absence of observed clinical sequelae: May be of concern and warrant further evaluation 1. EMA Guideline on similar biological medicinal products containing monoclonal antibodies non-clinical and clinical issues, May 2012; 2. FDA Guidance for Industry. Scientific Considerations in Demonstrating Biosimilarity to a Reference Product. HHS FDA/CDER/CBER, Apr
![RWE, non-medical change in anti-tnf therapy in IBD IBD Comparison group vs continued reference product Powered to detect differences in efficacy or safety (sample size of switched cohort [n])](/docs-images/93/112369062/images/32-0.jpg "Follow-up after switch Patient-level reporting of outcomes Immunogenicity assessment Buer L, et al 1 (Norway) Sieczkowska J, et al 2 (Poland) Smits L, et al 3 (Netherlands) Díaz Hernández L, et al 4")
32 RWE, non-medical change in anti-tnf therapy in IBD IBD Comparison group vs continued reference product Powered to detect differences in efficacy or safety (sample size of switched cohort [n]) Follow-up after switch Patient-level reporting of outcomes Immunogenicity assessment Buer L, et al 1 (Norway) Sieczkowska J, et al 2 (Poland) Smits L, et al 3 (Netherlands) Díaz Hernández L, et al 4 (Spain) No all patients switch No (143) 6 months No Yes No all patients switch No (32) 8 months No No No all patients switch No (83) 12 months No Yes No all patients switch No (72; CD=62, UC=10) 6 months No No All studies observational not randomized at time of switch All studies contained a single switch Experience currently limited to switching from Remicade to Celltrion s CT-P13 (Inflectra /Remsima ) *Includes bio-naïve or previously TNFi exposed pts IBD, inflammatory bowel disease. 1. Buer L, et al. J Crohn's Colitis 2017;11: ; 2. Sieczkowska J, et al. J Crohn s Colitis 2016;10:127 32; 3. Smits L, et al. ECCO 2016 Abstract DOP030; 4. Díaz Hernández L, et al. ECCO 2016 Abstract P449 32
33 RWE, non-medical change in anti-tnf therapy in IBD Study Study Type Results Author Conclusions Buer L, et al 1 (Norway) Prospective, observational 97% (138/143) pts remained on CT-P13 at 6 mos (1 o EP) No significant changes in disease activity after switch 17 AEs (3 UC, 14 CD) 5 pts had ADAbs including 2 at BL Switching from Remicade to CT-P13 was feasible in a real-life population It was well tolerated with few AEs, including very limited ADAb formation and loss of response Sieczkowska J, et al 2 (Poland) Prospective study (pediatrics) Pts in remission: 69% at switch and 80% at last follow-up PCDAI activity score: 8.8 at switch; 6.6 at final follow up (P<0.05) All pts with CD (n=4) presented with clinical remission at final assessment 20 AEs reported in pts with CD; 3 in patients with UC Treatment with Remicade and CT-P13 produces similar results However, head-to head comparison is needed to confirm findings Smits L, et al 3 (Netherlands) Prospective, observational Median change in disease activity: CD: 0 ( 9 to +15, n=49); UC/IBD-U: 0 ( 4 to +4, n=19) FCP and CRP levels did not significantly change 5 AEs resulted in discontinuations 7 pts demonstrated detectable ADAbs (5 detectable at BL) These 1-year data suggest that switching IBD pts from Remicade to CT-P13 is feasible Díaz Hernández L, et al 4 (Spain) Retrospective, observational At 6 months, 86% of the pts (62/72) were in clinical remission 5 adverse events were recorded Switching to CT-P13 was effective in the maintenance clinical remission at 6 mos of treatment No relevant AEs were observed The use of the biosimilar supposed a cost saving in the treatment *Switched cohort studies: Studies including only one group, all patients are switched; PDCAI, Pediatric Crohn's Disease Activity Index Calculator ADAbs; antidrug antibodies; AE, adverse event; BL, baseline; CD, Crohn s disease; CRP, C-reactive protein; FCP, fecal calprotectin; IBD, inflammatory bowel disease; PCDAI, Pediatric Crohn's Disease Activity Index; UC, ulcerative colitis. 1. Buer L, et al. J Crohns and Colitis 2017;1: ; 2. Sieczkowska J, et al. J Crohns Colitis 2016;10:127 32; 3. Smits L, et al. ECCO 2016; Abstract DOP030; 4. Díaz Hernández L, et al. ECCO 2016; Abstract P449; 33
34 RWE of non-medical anti-tnf change in rheumatoid arthritis RA Nikiphorou E, et al 1 (Finland) Tweehuysen L, et al 2 (Netherlands) Gentileschi S, et al 3 (Italy) Scherlinger M, et al 4 (France) Avouac J, et al 5 (France) Comparison Group vs Continued Ref. Product Powered to Detect Differences in Efficacy or Safety (Sample Size of Switched Cohort [n]) Follow-up After Switch Patient-level Reporting of Outcomes Immunogenicity Assessment No all patients switch No (39) 11 mos (median) PROs No (only at BL) No all patients switch No (192) 6 mos No Yes No all patients switch No (23) 6 mos No No No all patients switch No (85) 43 wks (median) No No No all patients switch No (179) 300 days (3 infusions) No No Glintborg B, et al 6 (Denmark, DANBIO) Yes (historical) No (802) 413 days PROs Yes Yazici Y, et al 7 (Turkey) No new starts No (switchers: 148; continuers: 2870) 6 mos No No *Switched cohort studies: Studies including only one group, all patients are switched; Multiple cohort studies: Studies include more that one group of patients, one group is switched one group is not BL, baseline; NMS, non-medical switching; RA, rheumatoid arthritis; RWE, real-world experience; TNF, tumor necrosis factor. 1. Nikiphorou E, et al. Expert Opin Biol Ther 2015;15: ; 2. Tweehuysen L, et al. ACR 2016; Abstr 627; 3. Gentileschi, S et al. Expert Opin Biol Ther 2015;16:1311 2; 4. Scherlinger M, et al. Presented at the 2016 annual meeting of the French Rheumatology Society; 5. Avouac J, et al. Presented at the 2016 annual meeting of the French Rheumatology Society; 6. Glintborg B, et al. Ann Rheum Dis 2017;Epub Ahead of Print; 7. Yazici Y, et al. ACR Abstr
35 RWE of non-medical anti-tnf change in rheumatoid arthritis and PsA Study Study Type Results Author Conclusions Tweehuysen L. et al 1 (Netherlands) Prospective RA and PsA: mean DAS28-CRP remained stable for 0 6 mos SA: mean BASDAI increased from 3.8 to 4.3 (P=0.01) Withdrawals: inefficacy 35 pts; AEs 23 pts; infusion reactions 2 pts No serious AEs ADAs were detected in 47% pts at baseline and 38% pts after 6 mos Majority of RA, PsA and SA pts can be switched to CT-P13 without changes in efficacy, safety and immunogenicity 23% pts discontinued, possibly explained by nocebo and/or attribution effects rather than pharmacological differences Experience Currently Limited to switching from Remicade to Celltrion s CT-P13 (Inflectra /Remsima ) *Switched cohort studies: Studies including only one group, all patients are switched ADA, anti-drug anibodies; AE, adverse event; AUC, area under the curve; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C-reactive protein; DAS, disease activity score; d/c, discontinuation; HR, hazard ratio; RA, rheumatoid arthritis; SA, spondyloarthritis; PsA, Psoriatic Arthritis; NMS, non-medical switching; RWE, real-world experience. 1. Tweehuysen L, et al. ACR 2016; Abstract 627; 2. Avouac J, et al. Presented at the 2016 annual meeting of the French Rheumatology Society; 3. Nikiphorou E, et al. Expert Opin Biol Ther 2015;15:
36 Tracking the imunogenecity
37 Arguments to demonstrate their importance Humanization of therapies Explanation of secondary failures Choice of therapy after 2 failure Demonstration of biosimilarity Continuous improvement


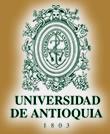
38 Protein 43-textbook-presentation
39 Hamze M et al. Front Immunol May 5;8:500.
40 Immunogenic Epitopes
41 Interaction HLA immunogenic peptides

42 Screening immunogenic peptides

43 Screening immunogenic peptides

44 Immunogenicity as a motivator for improvement
45 x INMUNOGENICIDAD Gracias