New Developments in the Lab Pharmacogenomics & Personalized Medicine Lab Developed Tests Molecular Microbiology. John T.
|
|
|
- Todd George
- 5 years ago
- Views:
Transcription
1 Saturday April 8, 2017 LD5 New Developments in the Lab Pharmacogenomics & Personalized Medicine Lab Developed Tests Molecular Microbiology John T. Daly, MD, FCAP Chief Medical Officer, COLA DESCRIPTION: The focus will be a discussion of molecular testing available including laboratory developed tests, molecular microbiology tools, and discussion of pharmacogenomics. OBJECTIVES: At the end of the session, participants will be able to: Explore new developments in drug therapy Consider advantages of personalized medicine Define Lab Developed Tests Recognize that changes to FDA-approved tests places them in high complexity category Describe complimentary roles of CMS and the FDA regarding the clinical laboratory Describe fundamentals of molecular technology Compare advantages of molecular microbiology over traditional technologies List examples of molecular microbiology products that can be used at point of care COLA Resources, Inc. and COLA do not endorse, directly or indirectly, the presentations given at this conference or the products or services provided by the exhibiting vendors. Presentations are intended to be free of bias. The use of any particular product is for demonstration purposes only, and does not imply an endorsement of the product by the presenter or the sponsors of the symposium CRI
2 2/19/2017 JOHN T. DALY, MD, FACP Drug administration today: basically a one size fits all model No simple way to distinguish responders and non-responders Diagnosis Drug Selection Ineffective Switch Drug Ineffective Another Switch and potentially on and on and on and on Drugs are developed for the average patient Clearly one size does not fit all 1
3 2/19/ ,000 Americans die annually and 2,000,000+ are hospitalized due to adverse reactions to medications Why does a given drug work for some and not all? Why does someone need twice the standard dose to be effective? Why do some patients exhibit side effects and others don t Right dose of Right drug for Right indication for Right patient at oright time 2
4 2/19/2017 Pharmacogenetics: Study of individual genedrug interactions, usually one or two genes that have dominant effect on a drug response (a simple relationship) Pharmacogenomics: Study of genomic influence on drug response, using multiple sites on the genome. Pharmacogenetics and pharmacogenomics enable prediction to be made of response to drugs based upon the individual genetic makeup Estimated that genetics can account for 20 95% of variability in drug disposition and effects Non-genetic factors include Age Organ function Concomitant therapy Drug interactions Nature of the disease 3
5 2/19/2017 Personalized medicine is based upon pharmacogenetics/genomics Enables use of pharmaceuticals based upon patient genome which allows greater predication of effectiveness Allows safer dosing actions Breast Cancer Patients 4
6 2/19/2017 Breast Cancer Patients Tumori cide Breast Cancer Patients 10 5
7 2/19/2017 No Effect/Hurt Helped Tumoric ide Why? Genetic variation leads to phenotypic differences and differences in how we all react to drugs. Having the receptor (protein) to recognize the drug HER2 receptors Other physiological traits that enable you to respond to a drug How drugs are processed in the body Enzymes in liver metabolize drugs 6
8 2/19/2017 Two Types of Breast Cancer Her2 - Her2 + Tumoricide is a personalized medication Tumoricide only works for Her2+ breast tumors No Effect/Hurt Helped Her2 - Tumorici de Her
9 2/19/2017 Given medication may be Active form that is then inactivated by metabolism of this active form Pro-drug that requires metabolism to produce an active metabolite There are four categories of metabolizers Ultra rapid metabolizers metabolize medications faster than normal Extensive metabolizers considered to have normal metabolism Intermediate metabolizers decreased rate of metabolism Poor metabolizers little to no ability to metabolize Drug given is active form that is inactivated by metabolism Ultra rapid metabolizers will require higher dose of drug to be effective Poor metabolizers will require a lower dose of drug to be effective and avoid toxicity Drug given is pro-drug requiring metabolism to produce the active medication Ultra rapid metabolizers will require a lower dose of drug to avoid toxicity Poor metabolizers will require a higher dose of drug to be effective (if it will be effective at all) 8
10 2/19/2017 CYP2D6 is an important gene in the metabolism of codeine Codeine is a pro-drug which is converted to morphine If individual is poor metabolizer codeine is ineffective If individual is an ultra-rapid metabolizer patients will receive too much morphine effect This is particularly important in children who can hallucinate, experience respiratory depression and develop other signs of overdose Today >120 drugs have pharmacogenomics information in their labeling information which indicate specific genes that influence patient response to drug This has led to development of companion diagnostics Companion diagnostics is a process that aligns the regulatory submission of a diagnostic test that provides information about the efficacy or potential efficacy of the simultaneously submitted drug submitted for FDA approval Goal is to stratify patients into groups that will respond to the particular pharmaceutical treatment 9
11 2/19/2017 Plasma based molecular diagnostic tests Tests are non-invasive Enables molecular genetic analysis from plasma cell free DNA Being used extensively in neo-natal work-ups and oncology Goal is to enable closer, more frequent monitoring and hopefully eliminate need for invasive biopsies While much discussed, technology is still in infancy Terminology in state of flux but cfdna and ctdna commonly seen Non-invasive pre-natal testing is one focus of cf technology but this is considered a screening test with false positive and negative results ctdna analysis is outgrowth of minimal residual disease work in CML and BCR-ABL gene rearrangements and drug imatinib Recent studies show ability to detect EGFR mutation in NSCLC up t0 16 weeks before visible radiologically 10
12 2/19/2017 JOHN T. DALY, MD, FACP COLA Chief Medical Officer Understand definition of laboratory developed tests Recognize that any changes in FDA approved tests places them in High Complexity Category Understand complementary roles of FDA and CMS in the clinical laboratory 1
13 2/19/2017 In-vitro diagnostic tests manufactured and used in a single laboratory Developed by hospitals, academic centers and clinical laboratories according to their own procedure LDT also referred to as in-house developed or home brew tests Often created in response to unmet clinical need of rare and emergent diseases or needs of small patient populations Used to diagnose and assess disease and disorders for which no FDA-authorized test-kit may not exists Currently used to detect or measure a wide variety of analytes and are important to continued development of personalized medicine Some are simple tests that measure a single analyte while others are complex and measure numerous analytes 2
14 2/19/2017 LDTs are considered high complexity under CLIA and all regulations related to high complexity must be met including personnel requirements Remember, if a change is made to the performance of an FDA approved test, that test is then considered to be a high complexity test FDA regulates manufacturers and devices to ensure that devices intended for use in diagnosis of disease are reasonable safe and effective and ensures clinical validity FDA functions under Federal Food, Drug and Cosmetic Act LDTs are considered devices as defined by FFDCA and therefore subject to FDA oversight although up until now FDA has not exercised enforcement Tests submitted to FDA for approval cannot have patient results reported until the FDA approval is received 3
15 2/19/2017 FDA review encompasses clinical validity and CLIA does not evaluate this While these agencies have different focus, scope and purpose, the two schemes are intended to be complementary Over the past 10 years there has been an explosive growth in numbers of LDTs, facilities performing them, advances in technology and changes in business models which has caused a re-evaluation of the oversight by the government Lack of evidence supporting the clinical validity of tests Deficient adverse event reporting No pre-market review of performance data Unsupported manufacturer claims Inadequate product labeling to provide information to patients and providers including test interpretation Lack of transparency Uneven playing field Threats to scientific integrity of clinical trials No comprehensive listing of all LTDs being used 4
16 2/19/2017 5
17 JOHN T. DALY, MD, FACP COLA Chief Medical Officer Review fundamentals of molecular technology Understand advantages of molecular microbiology when compared with traditional technologies Introduce examples of newer molecular microbiology products that can be used at point of care 2 1
18 Use of molecular tools in clinical microbiology laboratory has exploded since late 80 s Molecular testing overcomes several issues inherent in traditional microbiology: Organism survival during transport Inability to isolate some organisms using traditional methods Difficulty in detection of organisms in specimens with low organism numbers Difficulties of species identification of certain genera Lower sensitivity of antigen detection methods (EIA, DIF) 3 Early on, need for separate areas for reagent preparation, specimen preparation, amplification and identification Need for molecular technologists and labor intensive procedures Cost of reagents and equipment However, new technology allows for multiplicity of steps to be performed on one analyzer with minimal human intervention Today cost and need for adequate volume to support instrument use is issue for the smaller laboratories 4 2
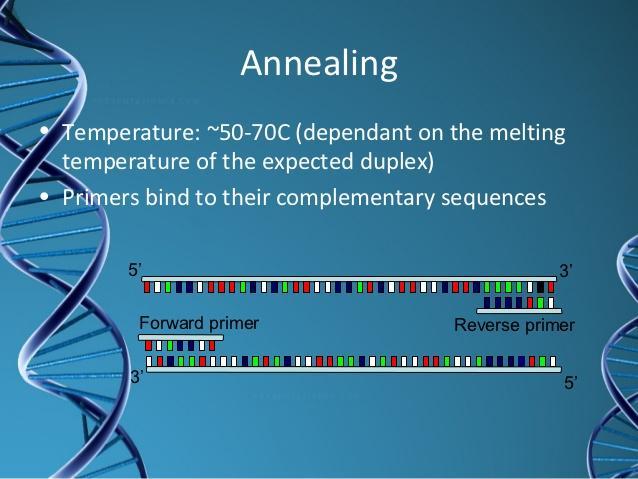
 Target Amplification (Polymerase chain reaction, Reverse transcription PCR) Amplification")
19 Signal Amplification Technology does not increase number of copies of target but rather signal probe attaches to a target DNA molecule and signal from attached probe is detected. If the probe is a nucleic acid with a fluorescent signal it is called FISH (fluorescent insitu hybridization) Target Amplification (Polymerase chain reaction, Reverse transcription PCR) Amplification of the nucleic acid sequence of interest geometrically replicates target into millions of copies which are then detected 5 6 3

20 7 8 4

21 RT-PCR amplifies RNA targets Portion of RNA genome transcribed into complementary DNA (cdna) and the cdna is then amplified Used extensively in RNA virus identification HIV, HCV, Influenza viruses
22 Among first organisms detected clinically were Chlamydia trachomatis and Neisseria gonorrhea Originally identified through signal amplification but target amplification rapidly followed Hepatitis B and C and HIV both qualitative and quantitative in mid 90 s and by 2005 in common usage 11 MRSA gene is meca and it has multiple variants meca can be present in both MRSA and CNS Multiplex assays used with multiple variants of the meca gene and S aureus orfx gene which can separate MRSA and CNS Self-contained cartridge systems available with all reagents needed and require minimal hands on time TAT of 1-2 hours can be achieved Interesting that CHROmagar provides TAT of 24 hours Highlights quandary of more rapid test with additional cost vs. more traditional test with in many instances same TAT 12 6
23 Not that long ago culture followed by monoclonal fluorescent staining was used to identify influenza virus Progressed to antigen detection kits using EIA or immuno-chromatographic membrane methods which had great variability in sensitivity Today availability of rapid molecular diagnostics including waived testing that avoid the false positive and negative results of the non-molecular methods 13 Cause of antibiotic associated diarrhea and pseudomembranous colitis Contains two toxins Toxin A (TcdA) an enterotoxin Toxin B (TcdB) a cytotoxin Originally believed toxin A more significant but today toxin B is recognized as producing more damage to intestinal cells 14 7
24 Culture: Takes four days and does not differentiate toxigenic from non-toxigenic Toxin Assay: EIA for toxins A and B Results in 15 minutes but tests lack sensitivity Glutamate dehydrogenase (GDH) assays: GDH enzyme produced by C. difficile Negative result associated with high negative predictive value Positive results not necessarily associated with toxin production 15 Cell Cytotoxicity Neutralization Assay: Filtrate of stool inoculated onto tissue culture cells If cells ball up examine tissue culture which has added antibodies If the second culture with added antibodies lacks cytotoxic effect, indicates presence of toxin Considered a gold standard Results require 48 hours Molecular Methods: PCR assay detects regulatory gene responsible for production of toxins A and B Test provides results in matter of hours 16 8


25
26 Panels Available Respiratory Viral Panel Blood Culture Identification Panel Gastrointestinal Panel Meningitis/Encephalitis Panel 19 Multiplex Real-Time PCR Assay Panels test for multiple targets simultaneously Methodology is real-time PCR (amplifying and detecting simultaneously) 20 10
27 One sample One test Multiple results 1.5-hour turnaround time 21 Viruses Coronavirus NL63 Coronavirus HKU1 Coronavirus 229E Coronavirus OC43 Human Metapneumovirus Human Rhinovirus/Enterovirus Influenza A Influenza A/H1 Influenza A/H Influenza A/H3 Viruses con t Influenza B Parainfluenza 1 Parainfluenza 2 Parainfluenza 3 Parainfluenza 4 Respiratory Syncytial Virus Bacteria Chlamydophila pneumoniae Bordetella pertussis Mycoplasma pneumoniae 22 11
28 Gram + Bacteria Enterococcus Listeria monocytogenes Staphylococcus Staphylococcus aureus Streptococcus Streptococcus agalactiae Streptococcus pyogenes Streptococcus pneumoniae Yeast Candida albicans Candida glabrata Candida krusei Candida parapsilosis Candida tropicalis Gram Bacteria Acinetobacter baumannii Haemophilus influenzae Neisseria meningitidis Pseudomonas aeruginosa Enterobacteriaceae Enterobacter cloacae complex Escherichia coli Klebsiella oxytoca Klebsiella pneumoniae Proteus Serratia marcescens Antibiotic Resistance meca - methicillin resistant vana/b - vancomycin resistant KPC - carbapenem resistant 23 Bacteria Campylobacter (jejuni, coli and upsaliensis) Clostridium difficile (toxin A/B) Plesiomonas shigelloides Salmonella Yersinia enterocolitica Vibrio (parahaemolyticus, vulnificus and cholerae) Diarrheagenic E. coli/shigella Enteroaggregative E. coli (EAEC) Enteropathogenic E. coli (EPEC) Enterotoxigenic E. coli (ETEC) lt/st Shiga-like toxin-producing E. coli (STEC) stx1/stx2 E. coli O157 Shigella/Enteroinvasive E. coli (EIEC) Viruses Adenovirus F 40/41 Astrovirus Norovirus GI/GII Rotavirus A Sapovirus (I, II, IV and V) Parasites Cryptosporidium Cyclospora cayetanensis Entamoeba histolytica Giardia lamblia 24 12
29 Bacteria Escherichia coli K1 Haemophilus influenza Listeria monocytogenes Neisseria meningitidis Streptococcus agalactiae Streptococcus pneumonia Fungi Cryptococcus neoformans/gattii Viruses Cytomegalovirus (CMV) Enterovirus Herpes simplex virus 1 HSV-1 Herpes simplex virus 2 HSV-2 Human herpesvirus 6 (HHV-6) Human parechovirus Varicella zoster virus (VSV) 25 Respiratory Viral Panel Nasal Wash Nasal Swab Sputum Respiratory specimen in Viral Transport Medium Gastrointestinal Panel Raw stool to be transferred to appropriate stool transport media Blood Culture ID Panel Positive Blood culture bottle Meningitis/ Encephalitis Panel CSF 13

30

31 Limited exposure of technologists to potentially hazardous bacterial isolates More rapid diagnosis More rapid therapy delivered to patients Potential reduction of morbidity and mortality Improved utilization of resources