The Cat s Out of the Bag: Microbiological Investigations of Acute Transfusion Reactions.
|
|
|
- Damian Melton
- 5 years ago
- Views:
Transcription
1 The Cat s Out of the Bag: Microbiological Investigations of Acute Transfusion Reactions. Philippe Lagacé-Wiens, MD FRCPC, DTM&H plagacewiens@sharedhealthmb.ca
2 COI declaration I have no conflicts, real or apparent, bearing on the subject matter of the educational day.
3 This copy is provided exclusively for research purposes and private study. Any use of the copy for a purpose other than research or private study may require the authorization of the copyright owner of the work in question. Responsibility regarding questions of copyright that may arise in the use of this copy is assumed by the recipient.
4 Objectives 1. Explain how blood product become contaminated with bacteria and what kind of bacteria contaminate blood products. 2. Describe the clinical presentation of transfusion reactions caused by bacterial contamination. 3. Explain the role of microbiology in investigating febrile transfusion reactions 4. In broad terms, interpret results from a culture investigation.
5 Transfusion-associated infections - Background Transfusion-associated infections are generally seen as a rare event in modern blood systems. Virus transmission (HBV, HCV, HIV, HTLV) are often considered of greatest relevance, but are essentially non-existent. <1 in 1,000,000 units post-screening may contain HCV or HIV. <1 in 100,000 units post screening may contain HBV (likely far lower now). Bacterial contamination of blood products is considerably more common, and has emerged as the greatest residual threat of transfusion-transmitted disease. Platelets: 1:1000 to 1:2000 contaminated with bacteria. Apheresis platelets: 1:100 to 1:1000 contaminated with bacteria. PRBC: 3-10:10,000 units Clin Microbiol Rev Jan; 18(1): Lancet Jan; 361(9352):
6 Transfusion-associated infections - Background Transfusion events related to bacterial contamination are rare compared to contamination rates. For RBCs reported occurrences are <1-10 events per million units. 0.1 to 0.7 fatalities per million units. For platelet products: ~10-13 per million whole blood platelets to ~70 per million apheresis platelets. 1-2 fatalities per million whole blood derived platelet units to 10 per million apheresis units. Both events and mortality for contaminated platelet recipients are likely inflated because most recipients are BMT, chemotherapy patients and severely immunocompromised. Clin Microbiol Rev Jan; 18(1): Clin Chem Lab Med 2008;46(7):
7 Sources of contamination Most contamination occurs during phlebotomy from skin flora. Coagulase negative staphylococci (S. epidermidis and others), Bacillus sp., Corynebacterium sp., Cutibacterium (formerly Propionibacterium sp.) etc. These organisms tend to be inhibited at 4ºC, but readily proliferate at room temperature. Contamination from Gram-negative bacteria is typically the result of asymptomatic bacteraemia in the donor. Y. enterocolytica Salmonella enterica. Some contamination by Gram-negative bacteria will occur as a result of environmental contamination: Serratia marscecens, Pseudomonas sp. Clin Microbiol Rev Jan; 18(1): Clin Chem Lab Med 2008;46(7):
8 PRBC contamination Prospective studies have show PRBC contamination rates vary from study to study. Most consistently between 0.1 and 0.2% of units. Transfusion events from contaminated PRBC tend to be more serious, and have higher fatality than other products. 58% of cases are fatal in one study, 33% in another. Clin Chem Lab Med 2008;46(7):
9 PRBC contamination PRBC units are typically stored refrigerated. Relevant bacterial contamination of PRBC units is typically with bacteria capable of surviving and growing at these temperatures. Common skin organisms are less commonly implicated in severe events related to contamination of PRBC units. Not cryotolerant, poor growth at this temperature. Cryotolerant Gram-negatives are the greatest concern and responsible for most fatalities. Yersinia enterocolytica, Serratia sp., Pseudomonas sp. Clin Microbiol Rev Jan; 18(1):
10 RBC transfusions bacterial contamination reactions by the numbers The most comprehensive study reviewed 38 instances of PRBC-associated events and 61 platelet associated events. For PRBC-related events: Gram-positive (Staphylococcus, Enterococcus, Bacillus, Cutibacterium sp. 44.7% with 6% mortality Gram negative (Escherichia, Klebsiella, Serratia, Yersinia, Enterobacter, Pseudomonas, Proteus). 55.3% with 33% mortality. Clin Microbiol Rev Jan; 18(1):
11 Platelet contamination Platelets are stored at room temperature. Skin contaminants become more relevant as they will grow and proliferate at these temperatures, resulting in potential serious transfusion reactions. Gram positive bacteria account for 67.3% of cases where an organism was identified (10% mortality). Gram negative organisms comparatively less common. 32.8% of cases with a 45% mortality. Clin Microbiol Rev Jan; 18(1):
12 Clinical presentation Presentation is variable and may be immediate or delayed. Depends on load of bacteria, type of bacteria, host factors. The typical presentation is a significant febrile reaction, with or without symptoms of shock. These are the criteria used for accepting a blood product for culture. Many reaction may be overlooked or more minor. Especially true of contamination with less virulent organisms. Investigations (and available data on symptoms) are biased by selection of more severe reactions.
13 Role of microbiology Microbiology play two roles in management of bacteria-associated transfusion reactions. Screening products for bacterial contamination prior to release from the central blood bank. Investigation of significant febrile transfusion reactions for bacterial contamination of units. Screening of platelet products takes place at Canadian Blood Services. Platelet components cultured after 36 hours of storage, and platelets held for a minimum of six hours after culture before release. Any unit showing growth will not be released. Cultures are incubated for six days. If they turn positive, any units still in-house will be discarded. If already released, receiving hospitals are notified of the positive culture. Investigation of significant febrile transfusion reactions for bacterial contamination takes place in Shared Health labs.
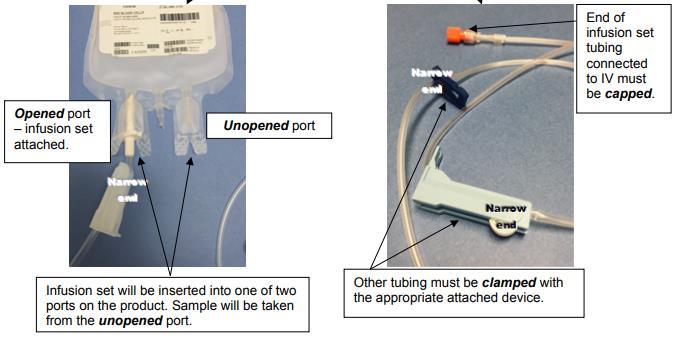
14 Investigation of bacterial contamination To trigger an investigation, certain clinical criteria must be met. 1ºC increase in body temperature compared to baseline AND a temperature >39ºC OR 1ºC increase in body temperature compared to baseline AND a temperature >38ºC and any of the following signs: Rigors Hypotension Tachycardia Dyspnea Shock Nausea or vomiting If criteria are met, a form CM105 must be filled out and submitted with the remaining blood product. Always clamp and cap the infusion set as leaking specimens will not be accepted.
15
16 Microbiology work-up Work-up depends on residual volume. All units submitted will have a direct stain performed. Contaminated units frequently have a high bacterial burden visible by direct stain. Available <1 hour after receipt by the lab. May provide critical information on patient management. Smear-positive specimens are also cultured directly to solid media for faster results. Blood products are cultured using the same instruments as blood cultures. Method provides a very high sensitivity (as little as one inoculated bacterium will lead to positive result) Small residual volume samples (<5mL) will have sterile broth added and cultured for aerobic an anaerobic bacteria. Larger volumes will have direct aerobic and anaerobic cultures. Final culture result takes 5 days. Positive cultures usually <2 days.
17 Patient samples Microbiological investigations of patients with transfusion reactions follow routine patient care practices. All patients with a significant febrile episode should have blood cultures drawn as soon as possible and prior to antibiotics. This should also be performed for significant febrile transfusion reactions. Blood cultures from patients with transfusion reactions should always be two sites, and two bottles from each site (aerobic and anaerobic)!! Additional investigations (imaging, cultures) depend on the clinical presentation. Confirming an alternative cause of a febrile episode assists in interpreting blood product investigation.
18 Reporting Blood product culture results are resulted in the same way all microbiology results are provided. In addition, the submitting blood bank will be copied. For smear or culture positive samples, the on-call physician for transfusion medicine will be notified by phone. Susceptibility testing results will be provided when available. Isolates will be retained in case molecular comparison studies are required to confirm a transfusion-related infection.
19 Confirming a transfusion-related bacterial infection Bacterial contamination transfusion-related event is considered probable if it meets the following criteria: Positive blood, blood component, or blood product culture. *Contamination of the blood sample or laboratory contamination is not suspected. The recipient presents signs and symptoms of sepsis with no other cause. The recipient's blood culture was not done. Or the recipient's blood culture is negative and the recipient was already taking antibiotics. Bacterial contamination is considered definite if it meets ALL of the following criteria: The same bacteria are found in the recipient and the blood, blood component, or blood product. The laboratory may need to perform molecular strain comparisons to achieve this for common organisms. *Contamination of the samples or laboratory contamination is not suspected.
20 Interpretation caveats Interpretation of blood product culture results can be challenging. Units can be contaminated with bacteria, but contamination may also occur during bag sampling and handling. Consider the following: What kind of product was it? Platelets are more likely to get contaminated than PRBCs, but are also screened. Plasma is kept frozen so bacterial growth doesn t occur and contamination is extremely rare. What type of organism? Gram-negative organisms are almost always real pathogens and likely came from the unit. Many Gram-positive organisms are contaminants and may also have contaminated the sample ports, bag and culture bottles. Is there an alternative cause to the febrile event? Was the blood product smear positive for bacteria? This confirms a unit with true bacterial contamination. How quickly did the culture become positive? Time to positivity <12 hours suggests a high load of bacteria in the sample. If an isolate is available from both the patient and unit, the lab can typically confirm that they are identical.
21 Questions?