Investigations in Immune Suppression for Monoclonal Antibody Therapeutics
|
|
|
- Alexis Bennett
- 5 years ago
- Views:
Transcription

1 Investigations in Immune Suppression for Monoclonal Antibody Therapeutics Vibha Jawa Principal Scientist AAPS NBC Meeting, May 2016 Clinical Immunology, Medical Sciences, Amgen
2 Background Therapeutic proteins (TP) may be immunogenic and can induce formation of anti-drug antibodies (ADA) Multiple biologics classes (e.g. proteins, nucleic acids and gene therapies) and modalities ( bispecifics, BiTes, fusion proteins ) can elicit anti-drug antibodies (ADAs) ADAs can pose challenges in both clinical and non-clinical settings during drug development. In the clinical setting, ADAs that develop against biotherapeutics can influence patient safety and interfere with product efficacy. ADA formation can impact the exposure and efficacy by modulating its pharmacokinetics (PK) properties and clearance via immune complexes Immune suppressive regimens have been established for treatment of certain diseases Successful immune tolerance induction to enzyme replacement therapy in CRIM-negative infantile Pompe disease
3 Experimental Design Phase 1 Explore existing immune suppressive regimens to mitigate the immunogenicity to biologics Understand how a concomitant immune suppression can impact immunogenicity to a fully human mab Develop a model to understand the magnitude of ADA formations and their effect on the pharmacokinetic profile of a therapeutic protein. Nonlinear mixed effects modeling will be used to relate the observed changes in mab exposure to the time-course and magnitude of the observed ADA formation. Phase 2 : Select the most appropriate regimen to confirm long term suppression after initial induction of tolerance Understand if a tolerance can be induced due to high dose of biologic
4 Phase 1 Objective/Questions Posed Explore immune suppressive regimens to mitigate the immunogenicity to biologics Understand how a concomitant immune suppression can impact immunogenicity Specifically Does immune suppression reduce the ADA incidence? Does immune suppression reduce ADA magnitude? Does immune suppression impact exposure?

5 IL-2 Targets of Immunosuppressant Drugs Activation Signal 1 TCR MHC II Peptide T cell APC CD28 B7.1/B7.2 G0/G1 Transition Enters Competent State T cell G1/S Transition Starts Proliferation Clonal Expansion Effector T cell Effector T cell Effector T cell
 (ml) (mg/ml) Treatment 1 6 SQ mab1 0.01,50 and 300 0.5 30 weekly 2 6 SQ mab1+ (FK506 and rapamycin) 0.01,50 and 300 (2mg/kg+ 6mg/kg ) 0.")
6 Dosing and Experimental Design of mab1 in Sprague Dawley Rats Group No. of Route / Test Article Dose Dose Dose Timing Animals Frequency Level Volume Conc. Of (mg/kg) (ml) (mg/ml) Treatment 1 6 SQ mab1 0.01,50 and weekly 2 6 SQ mab1+ (FK506 and rapamycin) 0.01,50 and 300 (2mg/kg+ 6mg/kg ) FK506 Co- administered with each dose Rapamycin dosed once with first dose of mab1 3 6 SQ mab1+ (MTX) 0.01,50 and 300 (5mg/kg) Day1 or first dosing ; Mtx 3 cycle regimen co- administered with 1 st dose, 24hrs and 48 hrs post 1 st dose Serum harvested for mab1 PK and ADA assessments

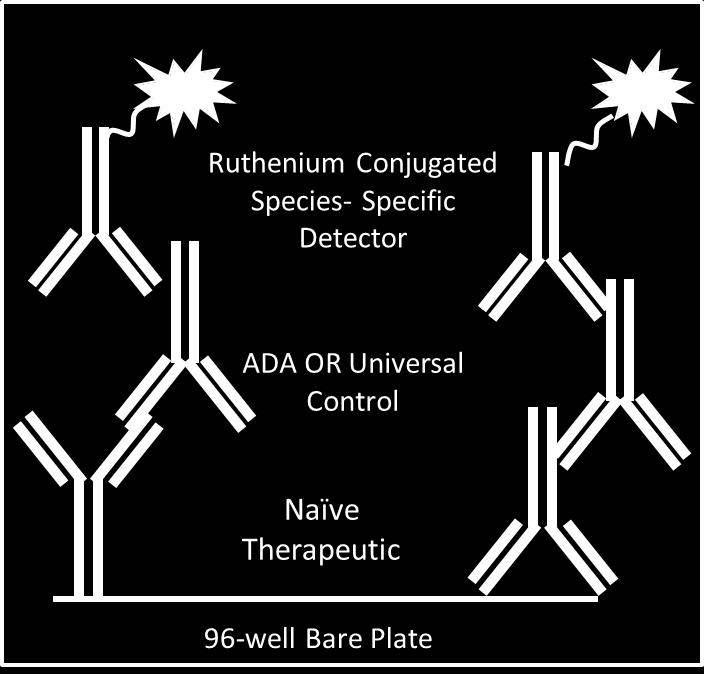
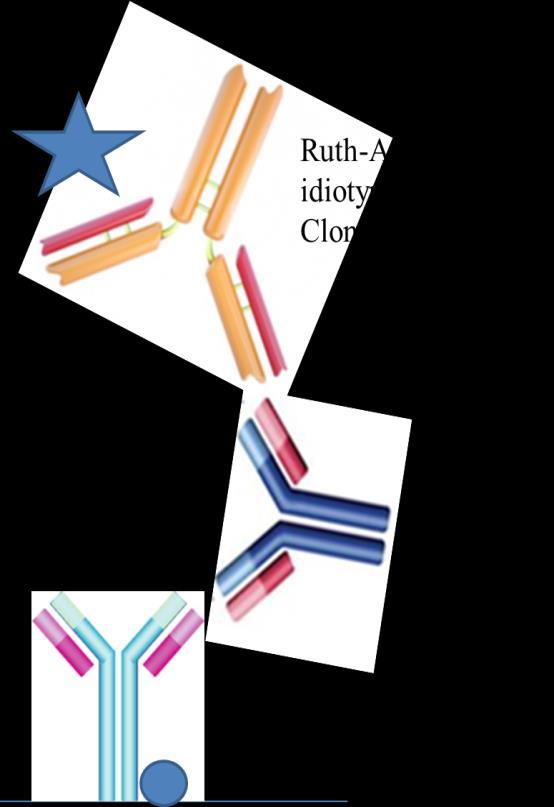
7 Immunogenicity and PK Testing Strategy ADA Screening ADA Specificity PK Analysis
8 DOES IMMUNE SUPPRESSION REDUCE THE ADA INCIDENCE?
9 % Incidence of ADA Positive Animals Suppression of CDR specific Immune Reactivity by Immune Suppressive Regimens following mab1 dosing 100% 90% mab1 Epitope 80% 70% 60% α-variable 50% 40% 30% 20% 10% 0% 0.01 mg/kg 50 mg/kg 300 mg/kg 0.01 mg/kg 50 mg/kg 300 mg/kg 0.01 mg/kg 50 mg/kg 300 mg/kg mab1 mab1 + FK506 + Rapamycin mab1 + Methotrexate Treatment and Dose Groups FK506 + Rapamycin more effective than Methotrexate in immune suppression Anti-CDR (variable ) response eliminated in FK506 + Rapamycin treated group and reduced in Mtx treated group
10 DOES IMMUNE SUPPRESSION REDUCE ADA MAGNITUDE?
11 Immune Suppression Regimens Reduce Magnitude of ADA response
12 DOES IMMUNE SUPPRESSION IMPACT EXPOSURE?
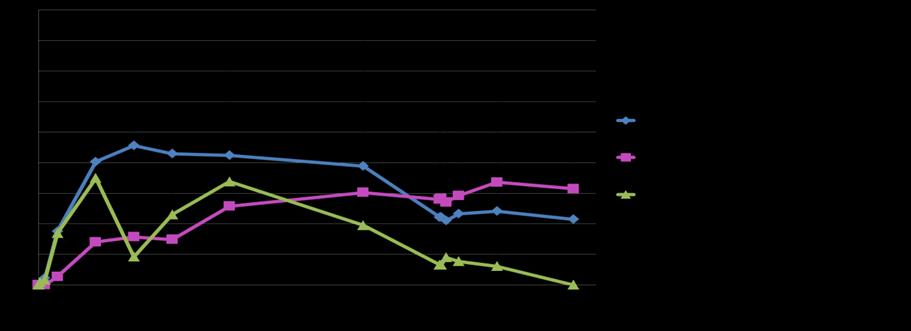
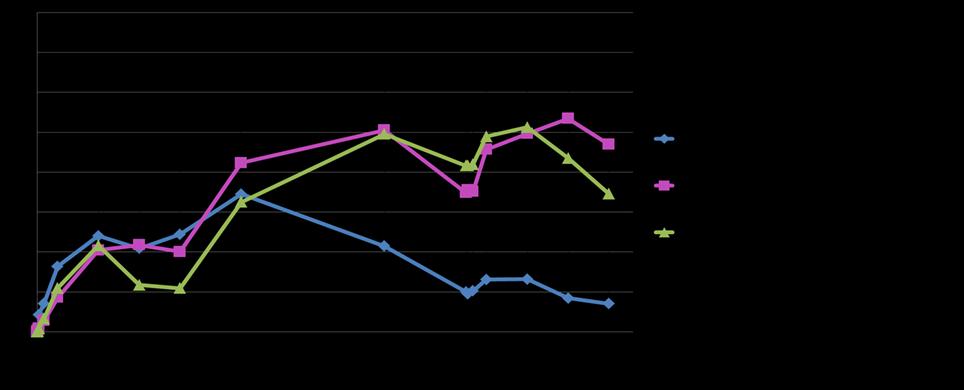
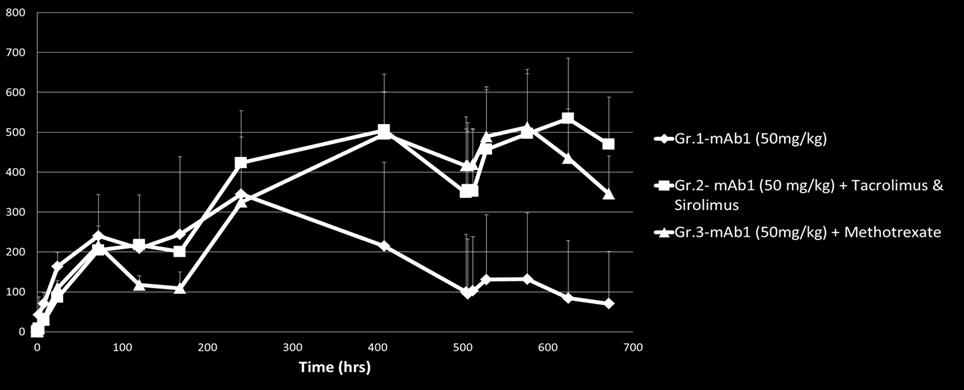
13 Immune Suppression Helps Retain Exposure
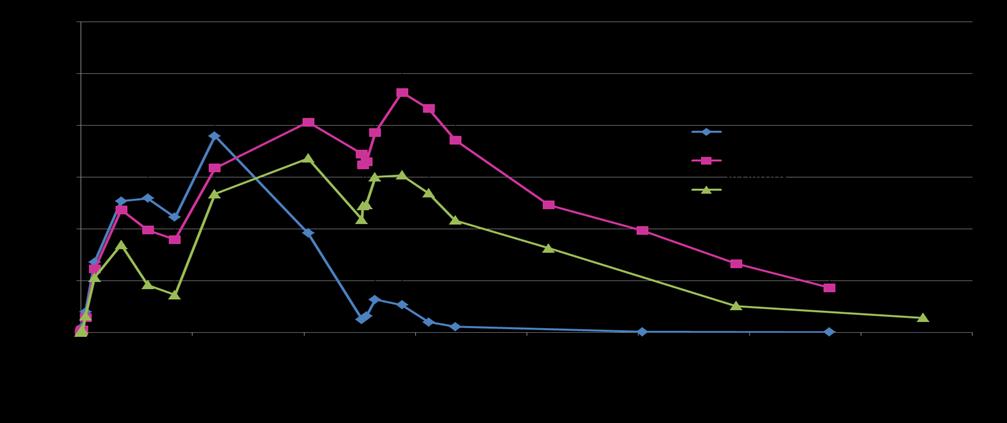
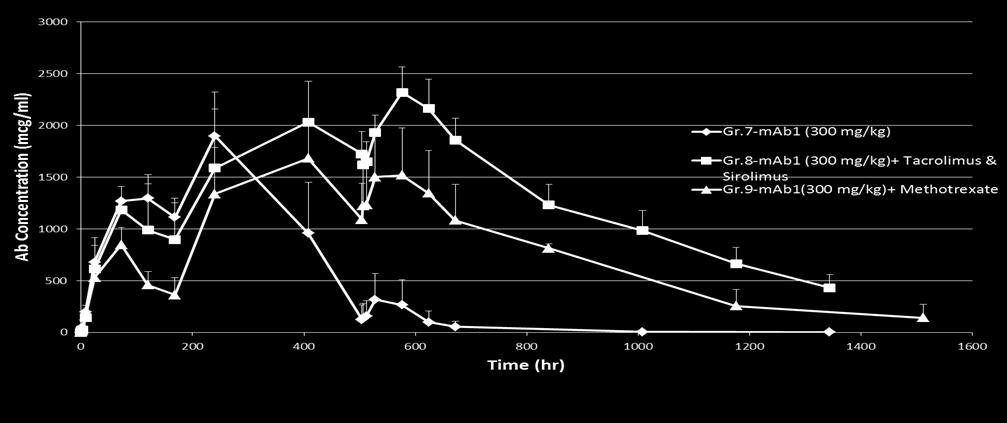
14 Immune Suppression Helps Retain Exposure
15 Immune Tolerance vs. Immune Suppression? Understand how concomitant immune suppressive treatments can change the immune response to biologics Immune tolerance or immunological tolerance is the state of unresponsiveness of the immune system to substances or tissue that have the capacity to elicit an immune response Regulatory T cells (Tregs) help maintain immunological unresponsiveness to self-antigens and suppressing excessive immune responses deleterious to the host.
: 43 49.")
16 IgG-derived Treg Epitopes J Clin Immunol Jan; 33( Suppl 1): IgG-derived Treg Epitopes
17 Conclusions Rapamycin and FK506 regimens were more effective in suppressing the unwanted immune response to biologic than Methotrexate regimen Methotrexate regimen was also effective in reducing the magnitude and overall incidence of immune response to a certain extent Some additional modifications in dosing and frequency needs to be addressed A reduction in immune response due to these regimens resulted in a more effective exposure to the biologic