Stem Cells: Evidence for Efficacy
|
|
|
- Olivia Richardson
- 5 years ago
- Views:
Transcription

1 Stem Cells: Evidence for Efficacy
2 Disclosures VA RR&D 1IK2RX A1 (PI: Harvey Smith) VA RR&D I01 RX (PI: Harvey Smith) Department of Veterans Affairs Medical Center, Philadelphia, PA FDA Orthopaedic Devices Panel

3 What is a Mesenchymal Stem Cell (MSC)? First described 1970s Lack of consensus on definition Flow cytometry and immunotyping frequently used as diagnostic criteria Differentiate into mesodermal cell lines capable of Osteogenesis Chondrogenesis adipogenesis
4 361 Exemption for Human Cells, Tissues, and Cellular and Tissue-Based Products The processing of minimally manipulated cells of structural tissues must: preserve original relevant characteristics of the tissue.. be intended for homologous use only.. may not be combined with another article.. the preparation must not be dependent on metabolic activity of living cells for its primary function processing that alters any relevant biological characteristics of cells or nonstructural tissues generally would be considered more than minimal manipulation Any other approach to cell therapy requires premarket approval or biological license application

5 55 patients partial medial meniscectomy Single injection 7-10 days postop Randomized to 3 groups 50x10^6 allogenic MSC 150x10^6 allogenic MSC Sodium hyaluronate vehicle control Evidence of Meniscus Regeneration Improved knee pain

6 Animal (hose) study 15mm defect trochlear ridge bilaterally Platelet-enhanced scaffold +/- stem cells delivered Arthroscopy 3 months post-op Tissue collected 12 months

7 Good results with APEF +/- BMSC At 3 months arthroscopic evaluation demonstrated good tissue At 12 months tissue appeared to be degenerating Tissue at 12 months generally fibrous 4/12 defects with APEF+BMSC developed bone The addition of BMSC to APEF did not appear to aid long-term repair
8 Treatment of knee arthritis/meniscectomy/chondral defect Trend towards single-stage procedures Expanded cells vs. Bone marrow concentrate for injection A carrier appears advantageous for open procedures : fibrin glue vs. HA MSCs have an anti-inflammatory effect that may confound outcome data MSCs appear to be safe in all published human cohorts/trials Addition of PRP/platelets has mixed findings : animal study suggests there may be potential for osteogenesis

9 Cryopreserved MSCs+Allograft does carry inherent risks There have been recall of lots with cryopreserved MSCs due to safety issues Same inherent risks of other cellular allogenic products
10 Animal Studies Disc Treatment with NP or Chondrocyte 14 Animal Studies using IVD or Chondrocyte Cell 7 used autologous cells 4 used allgeneic cells 3 used xenogeneic cells 12/14 studies demonstrated treatment effect Gross morphological or histological assessment Increased matrix deposition 7/14 studies positive radiology outcomes improved 8 studies demonstrated viability of cells up to 8 months Cell Source Autologous Allogeneic Xenogeneic Total Studies Intervertebral Disc Cells Stem Cells Animal Models Number of Studies Mouse Rat Rabbit Pig Dog Goat Sheep Articular Chondrocytes
11 Animal Studies Disc Treatment with Stem Cells 38 Animal Studies using stem cells 10 used autologous stem cells 16 studies used allgeneic cells 12 used xenogeneic cells Bone marrow derived MSCs most commonly used More variation in results Approximately ½ studies positive findings Varying survival times of cells following transplantation Cell Source Autologous Allogeneic Xenogeneic Total Studies Intervertebral Disc Cells Stem Cells Animal Models Number of Studies Mouse Rat Rabbit Pig Dog Goat Sheep Articular Chondrocytes
12 Clinical Trials Four published clinical reports EuroDisc Significantly less back pain and increased NP T2 signal at 2 years Case report of two patients (autologous MSCs) Pilot study 10 patients with autologous MSCs with good results Pilot study HSCs in 10 patients with poor results
13 Trajectory Based Tissue Engineering Growth trajectory of an engineered tissue Slow, fast, plateau Growth state Current modulus E Y (kpa) Time (wks) Adapted from Fisher+ 2013
14 Trajectory Based Tissue Engineering Growth trajectory of an engineered tissue Slow, fast, plateau Growth state Current modulus Growth rate Fit exponential to trajectory, differentiate curve for maximum slope E Y (kpa) de Y /dt (kpa/wk) 600 Data Model Fit Time (wks) Time (wks) Adapted from Fisher+ 2013
15 Trajectory Based Tissue Engineering In vitro cartilage defect model Adapted from Fisher+ 2013
16 Trajectory Based Tissue Engineering In vitro cartilage defect model Growth state does not correlate to integration strength Int. Strength (kpa) R² = Eq. Comp. Mod. (kpa) Adapted from Fisher+ 2013
17 Trajectory Based Tissue Engineering In vitro cartilage defect model Growth state does not correlate to integration strength Growth rate does correlate Int. Strength (kpa) R² = Eq. Comp. Mod. (kpa) Int. Strength (kpa) R² = de/dt (kpa/wk) Adapted from Fisher+ 2013




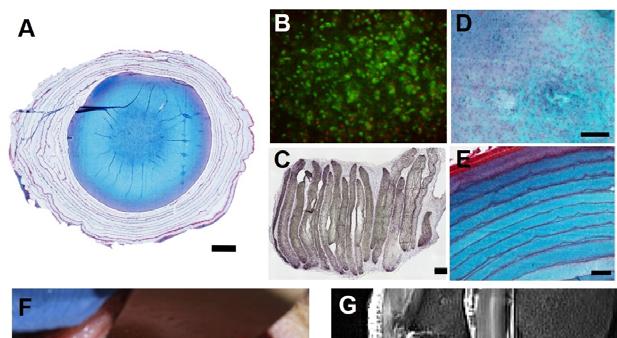
 0 VB EP EP 250µm")

 DA edap PS S")


 DA edap")
18 Figure 6 d a AF/NP edaps Mecha nics M Histol R ogy I Week 1 Week 2.5 Week 5 VB AF EP Week -5 Week -3 Week 0 Wee k 1 Week 2.5 Wee k 5 AF N P A See F AF, dnp Comb AF, ine NP, EP Implan t b EP NP AF EP c Week 1 Week 2.5 Week 5 Average T2 (ms) Week 5 (Interfaces) 0 VB EP EP 250µm Week 1 edaps % difference T2 from NP DAPS AF Region Region f 10 5 Week 2.5 Week 5 Compressive Modulus (MPa) DA edap PS S native + e NP EP VB Week 5 1mm 50 µm AF AF Week 5 Week 5 (Interface) Week 5 (Interface) VB EP EP AF 100 µm native Toe Region 5 native 0 Transitio n Strain (%) DA edap PS S Linear Region native * Maximu m



19
20 So what is the evidence If you re a rat, rabbit, or goat with DDD we can help you For humans: No real evidence that current marketed injections and treatments effect the long-term outcome Manipulated/expanded injections of disc cells may effect disc proteoglycan content and cell content at up to 2 years Not clear if pain response (EuroDisc) are due to structural/cellular changes or to paracrine/antiinflammatory effects The future role is likely a better diagnostic modality for intradiscal pathology and then early intervention with NP cells or MSC cells that are pre-differentiated and manipulated