Platelet transfusion therapy. Orieji Illoh, M.D. January 23, 2007
|
|
|
- Monica Burns
- 6 years ago
- Views:
Transcription
1 Platelet transfusion therapy Orieji Illoh, M.D. January 23, 2007
2 The Eighteenth Century Transfusions were done only sporadically, and were generally animal to human. Transfusion was generally thought of as a cure for mental aberration or as a youth potion for the aged, rather than as a treatment for blood loss. Reciprocal transfusions were suggested as a cure for marital discord. Blood was thought to carry the characteristics of the donor to the recipient: sheep blood would make a dog grow wool, hooves, and horns; cat blood would make a girl feline, etc.

3 The Platelet Size: 1.5-3um Anuclear, discoid cell Circulating life span: 9-10 days, about 4-5 days when infused. Platelet count: 130, , ,000/uL are consumed daily for routine plugging of minor endothelial defects
4 The Role of platelets in hemostasis Formation of the platelet and fibrin plug Stages include Platelet adhesion Platelet activation and secretion Platelet aggregation Platelet associated coagulation Clot retraction and wound healing

5 Platelet adhesion, activation, aggregation and thrombus formation on subendothelial surface at an injured blood vessel. Stefan Offermanns. Molecular pharmacology encref.springer.de/ mp/ gif

6 Platelet Activation

7 Platelet Activation colorized scanning electron microscope image of platelets in various stages of activation

8 The platelet product 2 basic types Whole blood derived (random donor platelets) Platelet pheresis (single donor platelets) WB Light spin Apheresis PRP Hard spin PPP platelets RBC PC RBC Whole blood derived platelets
9 Random donor and Platelet pheresis Random donor $ $ Minimum amount: 5.5x10 10 /unit 8x10 7 leukocytes, <1ml RBC volume: ml Maximal availability, Easy to collect Dose escalation possible Multiple donor exposures Matching not practical High RBC and WBC content Platelet pheresis (Single donor) $$$ Minimum amount 3.0 x /unit leukocytes, rare RBC Volume: ml Single donor exposure Matching is possible Low RBC and WBC content Limits platelet dose Limited availability Inconvenient for donor
10 Storage Platelets were stored in the cold (1-6 o C) in the 1950s and 1960s Cold temperatures decrease platelet survival after transfusion Platelets loose their discoid shape and become spherical when damaged by the cold Cooling causes clustering of the von Willibrand factor receptor complexes facilitating ingestion by hepatic macrophages
11 Storage Suspended in plasma and anticoagulant or platelet additive solutions. Acid citrate dextrose is the anticoagulant of choice At degrees Constant agitation To prevent platelet activation and facilitate gas exchange Buffer to prevent drop in ph Permeable plastic containers Stored for 5 days

12 Infected platelet unit
13 In attempt to prevent bacterial contamination AABB- requires strategies to prevent bacterial inoculation and detection of bacterial growth during storage (since March 2004) We use the ph test on random donor units Blood center performs cultures on apheresis units

14 Platelet culture
15 The platelet storage lesion Decreased recovery and survival Altered morphology- decreased MPV, loss of disc shape, fragments apoptosis Altered glycoprotein Ib Decreased content of a granules and dense bodies (due to platelet activation) Decreased function Lactic acid from glycolysis Decreased ph
16 The future of platelet storage Modifying platelets with galactose Use of inhibitors of actin filament assembly Use of calcium chelators Freezing Pathogen reduction technology
17 Selection of platelets for transfusion ABO antigens are weakly expressed on platelets Can transfuse regardless of ABO type Most adults will neutralize soluble antigenic A or B substances ABO compatible units for smaller patients or repeated transfusions? Screen for anti A1 or anti B titers Volume reduce
18 Rh compatibility Rh antigens are not expressed on platelets Passenger red blood cells may lead to alloimmunization to red cell antigens Adhere to Rh type in women of childbearing potential or issue Rh immunoglobin
19 Selection of platelets for transfusion May need to pool random donor platelets Must be transfused within 4 hours Other modifications CMV reduced risk Leukocyte reduced Irradiated Volume reduced washed
, 651")
20 Volume reduced platelets Transfusion 45 (5),
21 Indications for Platelet transfusion Prophylactic transfusion Severe thrombocytopenia Before invasive procedure if thrombocytopenia is present Thrombocytopenic bleeding Dilutional thrombocytopenia Thrombocytopathy
22 Severe thrombocytopenia Most often seen in bone marrow failure Acute leukemia Acute promyelocytic anemia Hematopoietic stem cell transplantation After chemotherapy Myelodysplasia Aplastic anemia Numerous studies have been done to determine the threshold at which to transfuse platelets
23 Relationship between platelet count and bleeding risk in thrombocytopenic patients all hemorrhagic manifestations skin, bleeding, and epistaxis excluded grossly visible hemorrhage Slichter, Trans. Med. Rev. 18: , 2004

24 Some studies Optimizing platelet transfusion therapy*1. Blood Reviews, Volume 18, Issue 3, Pages J. Heal, N. Blumberg
25 Current practice Threshold of 10 x 10 9 /L in the absence of risk factors Risk factors include sepsis, bleeding, use of antibiotics, other hemostatic problems Threshold of 20 x 10 9 if risk factors exist May need to manage on an individual basis in chronic stable thrombocytopenia
26 Invasive procedures Studies suggest that invasive procedures can be performed safely with a platelet count of 50,000/uL Higher threshold for neurosurgical and ophthalmic procedures (100,000/uL) Can perform bone marrow biopsies in patients with severe thrombocytopenia without platelet support
27 Thrombocytopenic bleeding Depends on site of bleed Higher threshold for CNS (100,000/uL) 50,000 or higher in other situations
28 Dilutional thrombocytopenia Occurs with massive transfusion Transfusion of colloids, crystalloids and RBC Replacement of one blood volume will reduce platelet concentration by half
29 Massive transfusion
30 Recommendations Only transfuse platelets if there is evidence of microvascular bleeding In many cases platelets are given prophylacticaly
31 Thrombocytopathy Congenital Glanzman s thrombasthenia Bernard Soulier syndrome Storage pool defects Scotts syndrome Platelet factor V deficiency Others Acquired Cardiopulmonary bypass Uremia Aspirin Clopidogrel (Plavix) Ticlopidine (Ticlid) Tirofiban (aggrastat) Abciximab (Reo Pro) Epifibatide (Integrillin)
32 In hereditary platelet function disorders DDAVP will be useful in most defects Platelet transfusions especially if bleeding and thrombocytopenic, keep hematocrit above 35% Corticosteriods, e- aminocaproic acid
33 Cardiopulmonary bypass Fall in platelet count Platelet function defect Studies do not support prophylactic transfusion, however, keeping the platelet count at 80, ,000 may be beneficial
34 Uremia Drop in platelet count Defect in platelet function Transfused platelets become defective Other therapeutic options available including DDAVP, cryoprecipitate, conjugated estrogens

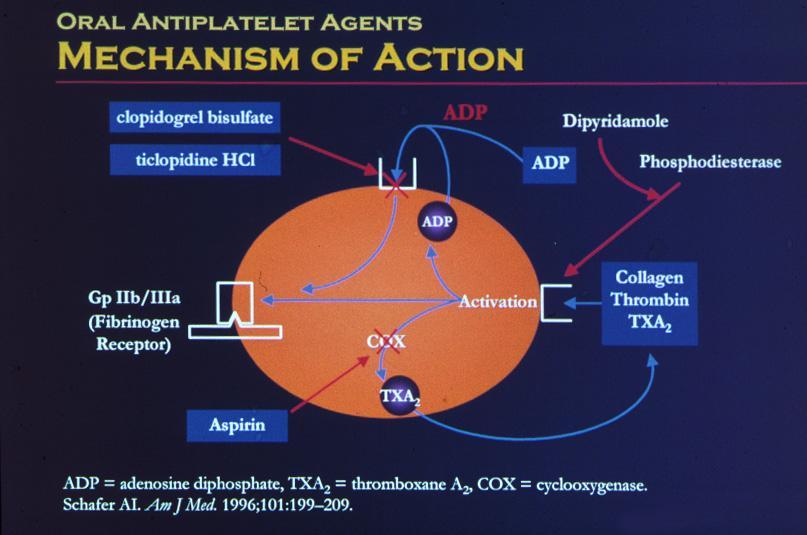
35 Activators of Platelets.
36
37 Aspirin Lack of Data but suggest platelet transfusion in bleeding due to aspirin Suggest stopping aspirin 3-10 days before surgery Studies have shown that people who went into surgery less than 3 days after stopping aspirin used more blood products
38 Plavix ( inhibits ADP induced aggregation) No consensus on when to stop the drug before surgery Patients with bleeding due to Plavix may have normal platelet counts Active metabolite persists after cessation of drug Therefore in a bleeding patient, may need platelet transfusions 4-5 day after stopping the drug
39 Ticlid ( inhibits ADP induced aggregation) Half life 4-5 days Effect on platelet is irreversible Delay elective surgery for several days if possible May use more blood products if drug is still present
40 Platelet glycoprotein IIb/IIIa receptor antagonists Aggrastat, ReoPro, Integrillin Do not permanently impair platelets Platelet function returns within several hours for aggrestat and integrillin and hours for Reo Pro May need platelet transfusion in emergencies
41 Selective Serotonin Reuptake inhibitors Used to treat depression and other mood disorders Case reports of increased bleeding risks Decreased platelet binding affinity Blockade of intraplatelet calcium mobilization Reduced platelet secretion in response to collagen Due to changes in the serotonin intraplatelet and plasma levels
42 Bleeding associated with SSRIs Usually not profound, superficial locations, Rarely require transfusions Hematomas, petechiae, bruising, epistasis Intracerebral, GI, retroperitonial bleeding has been reported Increased risk of perioperative bleeding
43 Splenomegaly May cause platelet sequestration Platelet transfusion rarely indicated
44 Immune thrombocytopenic purpura Platelet transfusion may be indicated in hemorrhagic emergencies (may need to hypertransfuse)
45 Contraindications to Platelet transfusion Autoimmune idiopathic thrombocytopenia purpura Thrombotic thrombocytopenia purpura Heparin induced thrombocytopenia Coagulopathy only Anatomic bleeding only
46 Standard Platelet doses Infants: 10ml/kg body weight Children: I unit (whole blood derived) for every 10-15kg body weight Adults: 4-8 units pooled or I unit pheresis

47 Expected Increment 1 unit 4 units 6 units 50lb 22,000/uL 88,000/uL 132,000/uL 100lb 11,000/uL 45,000/uL 66,000/uL 150lb 7,400/uL 30,000/uL 44,000/uL 200lb 5,500/uL 22,000/uL 33,000/uL
48 Assessment of response Cessation of hemorrhage Post transfusion count Dependent on size Initial platelet count Dose given One third transfused platelets will remain in the spleen
49 Corrected count increment (CCI) Takes into account the body surface area of the patient Need to obtain platelet count within 10 minutes to 1hour of transfusion CCI = platelet increment/ul x BSA (m 2 ) number of platelets transfused(x10 11 )
50 CCI Expected CCI should be > 7500 If less than 7500 on at least 2 occasions, the patient is declared refractory to platelet transfusions
51 Platelet refractoriness Immune Non Immune
52 Non Immune Causes Platelet quality: dose, washed, filtered Platelet age: slightly better increments with fresh platelets Massive bleeding Splenomegaly DIC Fever Bone marrow transplantation Graft vs host disease Amphotericin TTP Other drugs
53 Immune causes ABO incompatibility HLA incompatibility HPA incompatibility Autoantibodies Drug induced antibodies Passively acquired antibodies
54 HLA Alloimmunization Platelets bear ~70% of whole blood load of class I HLA-A and HLA-B antigen Do not express class II antigens Donor leukocytes (have both class I and II) provide a source of antigen presenting cells Hence the usefulness of leukocyte reduction!
55 TRAP Study Population: patients with newly diagnosed AML Control group received random platelets Treatment group Pooled platelets leukocyte reduced by filtration Pooled platelets with ultraviolet irradiation Apheresis platelets- leukocyte reduced All RBC units were leukocyte reduced

56 TRAP study Less HLA alloimmunization in all treatment groups compared to the control group No differences between study groups Low incidence of bleeding in all groups Recommend filtered components for all AML patients



57 Leukocyte reduction Achieved by filtration or UV irradiation Less than 5 x 10 6 leukocytes Filters will remove 99.9% leukocytes
58 Management of Platelet refractoriness Non Immune Treat or eliminate cause Transfuse platelets only if necessary
59 Management of Platelet refractoriness Immune causes Give ABO compatible platelets HLA alloimmunization HLA matched platelets HLA antigen mismatch Platelet crossmatch Unselected platelets
60 ABO compatible platelets Especially a problem in recipients with high titers of anti A or anti B ABO density on platelets might be a contributing factor A2 platelets contain 40 fold less of A antigen Pathogenesis: formation of immune complexes with soluble A and B substance Try ABO compatible
61 HLA alloimmunization Usually occurs 3-4 weeks after first transfusion Following pregnancy
62 HLA matching Improves platelet recovery Need to know patient and donor HLA type antibody specificity Can grade HLA matching based on number of antigens matched 80% patients will benefit
63 HLA antigen mismatch Characterize patient antibody Give platelets negative for the antigen
64 Return to unselected platelets HLA antibodies may disappear after one week to several months
65 Platelet crossmatch Can select concentrate irrespective of nature of alloimmunization Use ABO compatible platelets Can select from a larger pool of donors Found to be equivalent to HLA matching Several methodologies available Solid phase red cell adherence, flow cytometry, immunofluorescence, complement fixation
66 Platelet crossmatch using solid phase technology Donor platelets Add patient plasma Add antibody coated RBC Positive crossmatch Negative crossmatch
67 When all fails in HLA alloimmunization Other causes? If you tried HLA matched, try crossmatched or the reverse Antifibrinolytics Massive platelet transfusion IVIG Plasmapheresis? Immunoadsorbtion Immunosuppressive therapy HLA stripped platelets Thrombopoetin and platelet growth factors
68 Alternatives to Platelet Transfusion Cytokines Recombinant human thrombopoietin Human recombinant IL-6 Interleukin 3 Interleukin 11 Amifostine Antifibrinolytics
69 Platelet substitutes Lyophilized or freeze dried fixed platelets Undergoing phase I and II studies Infusible platelet membrane Can reduce bleeding time, under development Modified autologous rbc with covalently bound fibrinogen or peptide sequences Fibrinogen coated albumin microcapsules (synthocytes) Polyamide microcapsules
70 Complications of Platelet transfusion Disease transmission Bacterial Viral Others Immune related Febrile non hemolytic transfusion reaction Allergic reactions Transfusion related acute lung injury Transfusion associated graft versus host disease
71 Summary Different platelet products available Storage time is a limitation for availability Transfusion thresholds exist but may vary with the patient Refractoriness can limit effectiveness Leukoreduction can reduce the risk of alloimmunization Several drugs can cause platelet dysfunction
Blood Product Utilization
 Who gets what & when Why not to give blood? Volume Expander For specific number (except as related to procedures) To patients with religious objections to blood transfusions Blood given only when necessary
Who gets what & when Why not to give blood? Volume Expander For specific number (except as related to procedures) To patients with religious objections to blood transfusions Blood given only when necessary
Blood Component Preparation and Therapeutic Utilization
 Blood Component Preparation and Therapeutic Utilization Prof. A. Pourazar Immunohematologist and Transfusion medicine School of Medicine, Isfahan University Of Medical Science IRAN Red Blood cells, Platelets
Blood Component Preparation and Therapeutic Utilization Prof. A. Pourazar Immunohematologist and Transfusion medicine School of Medicine, Isfahan University Of Medical Science IRAN Red Blood cells, Platelets
Platelet Refractoriness: The Basics. Martin H. Bluth, MD, PhD
 Platelet Refractoriness: The Basics Martin H. Bluth, MD, PhD Complete Toxicology Laboratories, LLC Objectives Define platelet refractoriness and associated conditions that may cause platelet refractoriness.
Platelet Refractoriness: The Basics Martin H. Bluth, MD, PhD Complete Toxicology Laboratories, LLC Objectives Define platelet refractoriness and associated conditions that may cause platelet refractoriness.
Category Storage Shelf Life Additional Criteria
 CE Update [blood banking/transfusion medicine] Blood Components for Hemostasis Jun Teruya, MD, DSc, and Glenn Ramsey, MD From the Department of Pathology, Northwestern University Medical School, Chicago.
CE Update [blood banking/transfusion medicine] Blood Components for Hemostasis Jun Teruya, MD, DSc, and Glenn Ramsey, MD From the Department of Pathology, Northwestern University Medical School, Chicago.
Manejo de la transfusión de plaquetas. Ileana López-Plaza, MD
 Manejo de la transfusión de plaquetas Ileana López-Plaza, MD Thrombocytopenia Common in ICU setting 25-38% with< 100,000/µL 2-3 % with < 10,000/µL Common etiologies Drug-induced: heparin, antibiotics,
Manejo de la transfusión de plaquetas Ileana López-Plaza, MD Thrombocytopenia Common in ICU setting 25-38% with< 100,000/µL 2-3 % with < 10,000/µL Common etiologies Drug-induced: heparin, antibiotics,
Blood Component Therapy and Apheresis
 Blood Component Therapy and Apheresis Dr. Debasish Gupta Program Director, CHF International TRANSFUSION THERAPY Used primarily to treat two conditions Inadequate oxygen carrying capacity because of anemia
Blood Component Therapy and Apheresis Dr. Debasish Gupta Program Director, CHF International TRANSFUSION THERAPY Used primarily to treat two conditions Inadequate oxygen carrying capacity because of anemia
Managing platelet refractory patients: case studies. Presented by Paul F. Lindholm, M.D.
 Managing platelet refractory patients: case studies Presented by Paul F. Lindholm, M.D. Platelet transfusion Thrombocytopenia/transfusion goals Prophylactic >10K/mL to prevent serious bleeding (prophylactic)
Managing platelet refractory patients: case studies Presented by Paul F. Lindholm, M.D. Platelet transfusion Thrombocytopenia/transfusion goals Prophylactic >10K/mL to prevent serious bleeding (prophylactic)
4/22/2015. Platelet antibody screen and crossmatch. HLA antibody testing methods. Matched platelet timeline. Lymphocytotoxicity. Luminex technology
 Managing platelet refractory patients: case studies Presented by Paul F. Lindholm, M.D. Platelet transfusion Thrombocytopenia/transfusion goals Prophylactic >10K/mL to prevent serious bleeding (prophylactic)
Managing platelet refractory patients: case studies Presented by Paul F. Lindholm, M.D. Platelet transfusion Thrombocytopenia/transfusion goals Prophylactic >10K/mL to prevent serious bleeding (prophylactic)
ABO, Rh, HLA Antibodies Issues with Whole Blood NANCY M. DUNBAR, MD MEDICAL DIRECTOR, BLOOD BANK DARTMOUTH-HITCHCOCK MEDICAL CENTER, LEBANON, NH, USA
 ABO, Rh, HLA Antibodies Issues with Whole Blood NANCY M. DUNBAR, MD MEDICAL DIRECTOR, BLOOD BANK DARTMOUTH-HITCHCOCK MEDICAL CENTER, LEBANON, NH, USA The Appeal of Whole Blood WHOLE BLOOD IN EXSANGUINATING
ABO, Rh, HLA Antibodies Issues with Whole Blood NANCY M. DUNBAR, MD MEDICAL DIRECTOR, BLOOD BANK DARTMOUTH-HITCHCOCK MEDICAL CENTER, LEBANON, NH, USA The Appeal of Whole Blood WHOLE BLOOD IN EXSANGUINATING
Platelet type bleeding: (vwd) - Petechiae, purpura, ecchymoses, bruising - Menorrhagia, hematuria, occult GI bleed - Gingival bleeding, epistaxis
 - Petechiae, purpura, ecchymoses, bruising - Menorrhagia, hematuria, occult GI bleed - Gingival bleeding, epistaxis") 1 Nadanotes.com 2 Nadanotes.com 3 Nadanotes.com Platelet type bleeding: (vwd) - Petechiae, purpura, ecchymoses, bruising - Menorrhagia, hematuria, occult GI bleed - Gingival bleeding, epistaxis Clotting
1 Nadanotes.com 2 Nadanotes.com 3 Nadanotes.com Platelet type bleeding: (vwd) - Petechiae, purpura, ecchymoses, bruising - Menorrhagia, hematuria, occult GI bleed - Gingival bleeding, epistaxis Clotting
Ch 13: Blood. What does blood do? Transport: Regulation: Protection:
 Ch 13: Blood What does blood do? Transport: Regulation: Protection: SLOs Describe the composition of plasma and list the major functions of plasma proteins. Map hematopoiesis, starting from a pluripotent
Ch 13: Blood What does blood do? Transport: Regulation: Protection: SLOs Describe the composition of plasma and list the major functions of plasma proteins. Map hematopoiesis, starting from a pluripotent
PLATELET GUIDANCE DOCUMENT
 Government of Newfoundland and Labrador Department of Health and Community Services Provincial Blood Coordinating Program PLATELET GUIDANCE DOCUMENT Office of Administrative Responsibility Director, Regional
Government of Newfoundland and Labrador Department of Health and Community Services Provincial Blood Coordinating Program PLATELET GUIDANCE DOCUMENT Office of Administrative Responsibility Director, Regional
Local vasoconstriction. is due to local spasm of the smooth muscle (symp. reflex) can be maintained by platelet vasoconstrictors
 can be maintained by platelet vasoconstrictors") Hemostasis Hemostasis ( hemo =blood; sta= remain ) is the stoppage of bleeding, which is vitally important when blood vessels are damaged. Following an injury to blood vessels several actions may help
Hemostasis Hemostasis ( hemo =blood; sta= remain ) is the stoppage of bleeding, which is vitally important when blood vessels are damaged. Following an injury to blood vessels several actions may help
Case 1. Case 1. Case 2. Case 2. Review of Bleeding Disorders Case 1
 Review of Bleeding Disorders Case 1 Robert I. Handin, MD Professor of Medicine, Harvard Medical School Hematology Division Brigham & Women s Hospital 20 year college student is home on spring break and
Review of Bleeding Disorders Case 1 Robert I. Handin, MD Professor of Medicine, Harvard Medical School Hematology Division Brigham & Women s Hospital 20 year college student is home on spring break and
The clinical utility of IPF in thrombocytopenia
 The clinical utility of IPF in thrombocytopenia Platelets platelets Platelets are the smallest blood cells which are released by cytoplasmic blebbing of megakaryocytes with an average size of 2um. Normal
The clinical utility of IPF in thrombocytopenia Platelets platelets Platelets are the smallest blood cells which are released by cytoplasmic blebbing of megakaryocytes with an average size of 2um. Normal
Session 1 Topics. Vascular Phase of Hemostasis. Coagulation Pathway. Action of Unfractionated Heparin. Laboratory Monitoring of Anticoagulant Therapy
 ~~Marshfield Labs Presents~~ Laboratory Monitoring of Anticoagulant Therapy Session 1 of 4 Session 1 Topics Review of coagulation and the vascular phase of hemostasis Unfractionated heparin Low molecular
~~Marshfield Labs Presents~~ Laboratory Monitoring of Anticoagulant Therapy Session 1 of 4 Session 1 Topics Review of coagulation and the vascular phase of hemostasis Unfractionated heparin Low molecular
Managing Massive Transfusions in diverse Patient Populations in a Non-Metropolitan Area
 Managing Massive Transfusions in diverse Patient Populations in a Non-Metropolitan Area SHAUNA M.M. STURGILL, LAURIE GILLARD LEARNING OBJECTIVES 1. Compare and contrast massive transfusion protocols for
Managing Massive Transfusions in diverse Patient Populations in a Non-Metropolitan Area SHAUNA M.M. STURGILL, LAURIE GILLARD LEARNING OBJECTIVES 1. Compare and contrast massive transfusion protocols for
Heparin Induced Thrombocytopenia. Heparin Induced Thrombocytopenia. Heparin Induced Thrombocytopenia. Temporal Aspects.
 Heparin Induced Eric Kraut, MD Professor of Internal Medicine The Ohio State University Medical Center Heparin Induced Heparin induced thrombocytopenia occurs in up to 5 % of patients receiving unfractionated
Heparin Induced Eric Kraut, MD Professor of Internal Medicine The Ohio State University Medical Center Heparin Induced Heparin induced thrombocytopenia occurs in up to 5 % of patients receiving unfractionated
Common Inherited Bleeding Disorders
 CAA 2015 Annual Conference Common Inherited Bleeding Disorders Bob Miller, A October 8, 2015 VWF has two jobs Loosely bound to protect FVIII and tether to site of injury All other coagulation factors also
CAA 2015 Annual Conference Common Inherited Bleeding Disorders Bob Miller, A October 8, 2015 VWF has two jobs Loosely bound to protect FVIII and tether to site of injury All other coagulation factors also
Vein-to-Vein: Creating New Products to Optimize Patient Outcomes
 Vein-to-Vein: Creating New Products to Optimize Patient Outcomes BETH H. SHAZ, MD CHIEF MEDICAL AND SCIENTIFIC OFFICER EXECUTIVE VICE PRESIDENT NEW YORK BLOOD CENTER N Y B C. O R G S A V E A L I F E N
Vein-to-Vein: Creating New Products to Optimize Patient Outcomes BETH H. SHAZ, MD CHIEF MEDICAL AND SCIENTIFIC OFFICER EXECUTIVE VICE PRESIDENT NEW YORK BLOOD CENTER N Y B C. O R G S A V E A L I F E N
ABO Typing Discrepancies
 Jayme Heimonen MT(ASCP)SBB Blood Bank Technical Specialist Borgess Medical Center Kalamazoo, MI ASCLS-Michigan 2016 1 Expected reactions are missing 4+ 0 4+ 0 0 0 0 0 4+ 0 0 3+ 2 Unexpected reactions are
Jayme Heimonen MT(ASCP)SBB Blood Bank Technical Specialist Borgess Medical Center Kalamazoo, MI ASCLS-Michigan 2016 1 Expected reactions are missing 4+ 0 4+ 0 0 0 0 0 4+ 0 0 3+ 2 Unexpected reactions are
Emergency and Perioperative Hemostasis Testing: Which Assays Provide Helpful Information. Wayne Chandler, MD Laboratory Medicine Seattle Children s
 Emergency and Perioperative Hemostasis Testing: Which Assays Provide Helpful Information Wayne Chandler, MD Laboratory Medicine Seattle Children s Emergency Hemostasis Testing Patients actively bleeding
Emergency and Perioperative Hemostasis Testing: Which Assays Provide Helpful Information Wayne Chandler, MD Laboratory Medicine Seattle Children s Emergency Hemostasis Testing Patients actively bleeding
Physiology Unit 3 HEMATOLOGY
 Physiology Unit 3 HEMATOLOGY In Physiology Today Hematocrit Percentage of blood volume that is erythrocytes 45% in men 42% in women Average blood volume in is 5 L Plasma Large amounts of organic/inorganic
Physiology Unit 3 HEMATOLOGY In Physiology Today Hematocrit Percentage of blood volume that is erythrocytes 45% in men 42% in women Average blood volume in is 5 L Plasma Large amounts of organic/inorganic
What s COLD is Hot Again!
 What s COLD is Hot Again! Back to the Future with Whole Blood D. Joe Chaffin, MD LifeStream Transfusion Medicine Forum March 9, 2019 Objectives Describe historical use of whole blood Outline current impetus
What s COLD is Hot Again! Back to the Future with Whole Blood D. Joe Chaffin, MD LifeStream Transfusion Medicine Forum March 9, 2019 Objectives Describe historical use of whole blood Outline current impetus
The Coagulation Workup In The Office Setting
 CAA Conference alm Springs 2012 The Coagulation Workup In The Office Setting CAA Conference alm Springs, October 2012 Robert Miller, A-C Henoch-Schoenlein urpura 1 CAA Conference alm Springs 2012 2 CAA
CAA Conference alm Springs 2012 The Coagulation Workup In The Office Setting CAA Conference alm Springs, October 2012 Robert Miller, A-C Henoch-Schoenlein urpura 1 CAA Conference alm Springs 2012 2 CAA
Clinical Use of Plasma for Transfusion. Irma Szymanski, MD Professor of Pathology, Emerita University of Massachusetts Medical School
 Clinical Use of Plasma for Transfusion Irma Szymanski, MD Professor of Pathology, Emerita University of Massachusetts Medical School PLASMA PRODUCTS FOR TRANSFUSION Fresh Frozen Plasma (FFP) Thawed Plasma
Clinical Use of Plasma for Transfusion Irma Szymanski, MD Professor of Pathology, Emerita University of Massachusetts Medical School PLASMA PRODUCTS FOR TRANSFUSION Fresh Frozen Plasma (FFP) Thawed Plasma
LABORATORY DIAGNOSIS OF BLEEDING DISORDERS
 LABORATORY DIAGNOSIS OF BLEEDING DISORDERS Primary & Secondary Hemostasis Disorders http://.columbia.edu/itc/hs/medical/selective/advclinicalpathology/2004/lecture/lab%20diagnosis%20of%20bleeding%20disorders.ppt
LABORATORY DIAGNOSIS OF BLEEDING DISORDERS Primary & Secondary Hemostasis Disorders http://.columbia.edu/itc/hs/medical/selective/advclinicalpathology/2004/lecture/lab%20diagnosis%20of%20bleeding%20disorders.ppt
Common Inherited Coagulation Disorders. Inherited Coagulation Disorders. All coagulation factors and platelets in circulation (unactivated)
") Common Inherited Coagulation Disorders Bob Miller, A 2017 Inherited Coagulation Disorders Brief review of coagulation Disorders related to platelet dysfunction (not the acquired thrombocytopenias) Disorders
Common Inherited Coagulation Disorders Bob Miller, A 2017 Inherited Coagulation Disorders Brief review of coagulation Disorders related to platelet dysfunction (not the acquired thrombocytopenias) Disorders
Transfusion effect of random donor platelet and single donor platelet in thrombocytopenic patients at tertiary care hospital of South Gujarat
 International Journal of Research in Medical Sciences Unagar CA et al. Int J Res Med Sci. 2017 Jul;5(7):3033-3037 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20172983
International Journal of Research in Medical Sciences Unagar CA et al. Int J Res Med Sci. 2017 Jul;5(7):3033-3037 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20172983
Blood is 55% Plasma (Liquid)
") Blood is 55% Plasma (Liquid) The plasma portion of blood is: 91% Water Maintains blood volume Transports molecules 7% Proteins (ie: clotting proteins, albumin, immunoglobulins ) 2 % Salts, gases (O 2,
Blood is 55% Plasma (Liquid) The plasma portion of blood is: 91% Water Maintains blood volume Transports molecules 7% Proteins (ie: clotting proteins, albumin, immunoglobulins ) 2 % Salts, gases (O 2,
Supplementary Online Content
 Supplementary Online Content Garban F, Guyard A, Labussière H, et al; Evaluation of the Efficacy of Platelets Treated With Pathogen Reduction Process (EFFIPAP) Study Group. Comparison of the hemostatic
Supplementary Online Content Garban F, Guyard A, Labussière H, et al; Evaluation of the Efficacy of Platelets Treated With Pathogen Reduction Process (EFFIPAP) Study Group. Comparison of the hemostatic
Disclosures. Thromboelastography. TEG Methodology. TEG Output. Thromboelastography (TEG): Basics & Clinical Applications
: Basics & Clinical Applications") Thromboelastography (TEG): Basics & Clinical Applications Paula J. Santrach MD Associate Professor, Laboratory Medicine Mayo Clinic Rochester, MN Disclosures Relevant financial relationships NONE Off label
Thromboelastography (TEG): Basics & Clinical Applications Paula J. Santrach MD Associate Professor, Laboratory Medicine Mayo Clinic Rochester, MN Disclosures Relevant financial relationships NONE Off label
Stem Cells and Multiple Myeloma
 Stem Cells and Multiple Myeloma What is Multiple Myeloma Multiple Myeloma is a cancer of your plasma cells, a type of white blood cell present in your bone marrow Plasma cells normally make proteins called
Stem Cells and Multiple Myeloma What is Multiple Myeloma Multiple Myeloma is a cancer of your plasma cells, a type of white blood cell present in your bone marrow Plasma cells normally make proteins called
Faculty Disclosure RONALD A SACHER, MD,FRCPC FCAP
 Faculty Disclosure RONALD A SACHER, MD,FRCPC FCAP On the speakers bureau of BAYER BIOLOGICALS(also a consultant); GLAXO SMITH KLINE AND ORTHO BIOTECH. 1 Faculty Disclosure Ronald A.Sacher, MD, FRCPC, FCAP
Faculty Disclosure RONALD A SACHER, MD,FRCPC FCAP On the speakers bureau of BAYER BIOLOGICALS(also a consultant); GLAXO SMITH KLINE AND ORTHO BIOTECH. 1 Faculty Disclosure Ronald A.Sacher, MD, FRCPC, FCAP
New Drug Therapies for ITP
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/new-drug-therapies-for-itp/3710/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/new-drug-therapies-for-itp/3710/
OVERVIEW OF LABORATORY DIAGNOSTIC TESTING FOR PLATELET DISORDERS
 OVERVIEW OF LABORATORY DIAGNOSTIC TESTING FOR PLATELET DISORDERS Catherine P. M. Hayward, MD PhD, FRCP(C) Head, Coagulation, Hamilton Regional Laboratory Medicine Program Professor, Pathology and Molecular
OVERVIEW OF LABORATORY DIAGNOSTIC TESTING FOR PLATELET DISORDERS Catherine P. M. Hayward, MD PhD, FRCP(C) Head, Coagulation, Hamilton Regional Laboratory Medicine Program Professor, Pathology and Molecular
CURRENT COURSE OFFERINGS
 The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
The American Red Cross offers regular educational opportunities as a convenient way for healthcare providers to receive relevant blood banking and transfusion medicine information. The bi-monthly sessions,
Alberta Health Services - Edmonton Zone Massive Hemorrhage Protocol
 This document applies to all Covenant and AHS sites. Client Resource 23: Alberta Health Services - Edmonton Zone Regional Laboratory Services This document is applicable at site(s): GNH MIS RAH SGH UAH
This document applies to all Covenant and AHS sites. Client Resource 23: Alberta Health Services - Edmonton Zone Regional Laboratory Services This document is applicable at site(s): GNH MIS RAH SGH UAH
PROVINCIAL BLOOD COORDINATING PROGRAM DEFINITIONS NLBCP-063
 Government of Newfoundland and Labrador Department of Health and Community Services Provincial Blood Coordinating Program PROVINCIAL BLOOD COORDINATING PROGRAM DEFINITIONS Office of Administrative Responsibility
Government of Newfoundland and Labrador Department of Health and Community Services Provincial Blood Coordinating Program PROVINCIAL BLOOD COORDINATING PROGRAM DEFINITIONS Office of Administrative Responsibility
Factor Concentrates. More is better? Alexander Duncan MD Emory Medical Labs
 Factor Concentrates. More is better? Alexander Duncan MD Emory Medical Labs Call from OR! Scenario -1 Patients is bleeding out! Don t ask why, what rate what s been done! We need blood now! What kind of
Factor Concentrates. More is better? Alexander Duncan MD Emory Medical Labs Call from OR! Scenario -1 Patients is bleeding out! Don t ask why, what rate what s been done! We need blood now! What kind of
Zarxio. Zarxio (filgrastim-sndz) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Zarxio Page: 1 of 5 Last Review Date: December 2, 2016 Zarxio Description Zarxio (filgrastim-sndz)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Zarxio Page: 1 of 5 Last Review Date: December 2, 2016 Zarxio Description Zarxio (filgrastim-sndz)
Blood transfusion in special situations and poly-trauma. Dr Marina Karakantza Consultant Haematologist in Transfusion Medicine, LTHT
 Blood transfusion in special situations and poly-trauma Dr Marina Karakantza Consultant Haematologist in Transfusion Medicine, LTHT Uncontrolled bleeding is a major preventable cause of death in trauma
Blood transfusion in special situations and poly-trauma Dr Marina Karakantza Consultant Haematologist in Transfusion Medicine, LTHT Uncontrolled bleeding is a major preventable cause of death in trauma
Index. Autoimmune thrombocytopenic purpura (AITP), 100, 102, 105, 108, 187 Automated platelet counters, , 108
, 100, 102, 105, 108, 187 Automated platelet counters, , 108") A Accuracy, 6, 7, 15, 46, 52, 53, 61, 75, 100, 143, 144, 149, 166, 176, 178 Acquired coagulation disorders, 111 115 Acquired platelet disorders, 99 108 ACT. See Activated clotting time (ACT) Activated
A Accuracy, 6, 7, 15, 46, 52, 53, 61, 75, 100, 143, 144, 149, 166, 176, 178 Acquired coagulation disorders, 111 115 Acquired platelet disorders, 99 108 ACT. See Activated clotting time (ACT) Activated
Guidelines for the use of blood warming devices(aabb) Reference: 2002 AABB
 Reference: 2002 AABB") Guidelines for the use of blood warming devices(aabb) Reference: 2002 AABB 1 Hypothermia Introduction Induced by rapid, large-volume transfusion of refrigerated blood components A potential source of serious
Guidelines for the use of blood warming devices(aabb) Reference: 2002 AABB 1 Hypothermia Introduction Induced by rapid, large-volume transfusion of refrigerated blood components A potential source of serious
Hemostasis. by Mohie-Aldien Elsayed
 Hemostasis by Mohie-Aldien Elsayed Hemostasis Hemostasis is defined as the process that maintains the flowing blood in a fluid state and confined to the circulatory system Coagulation prevents excess blood
Hemostasis by Mohie-Aldien Elsayed Hemostasis Hemostasis is defined as the process that maintains the flowing blood in a fluid state and confined to the circulatory system Coagulation prevents excess blood
2017 AABB Annual Meeting On-Demand SAM Sessions
 2017 AABB Annual Meeting On-Demand SAM Sessions The following 14 SAM sessions from the 2017 AABB Annual Meeting are eligible for up to 17.75 SAM eligible credits. The number of credits is based on the
2017 AABB Annual Meeting On-Demand SAM Sessions The following 14 SAM sessions from the 2017 AABB Annual Meeting are eligible for up to 17.75 SAM eligible credits. The number of credits is based on the
Using TEG in the ED, OR, and ICU. Don H. Van Boerum, MD, FACS
 Using TEG in the ED, OR, and ICU Don H. Van Boerum, MD, FACS Trauma Surgeon, Director of Surgical Critical Care, Co-Director of Shock Trauma ICU, Intermountain Medical Center, Intermountain Healthcare
Using TEG in the ED, OR, and ICU Don H. Van Boerum, MD, FACS Trauma Surgeon, Director of Surgical Critical Care, Co-Director of Shock Trauma ICU, Intermountain Medical Center, Intermountain Healthcare
ANEMIA. Oral iron. IV iron gluconate (order set #233)
") PREVENTION ANEMIA Oral iron IV iron gluconate (order set #233) TRANSEXAMIC ACID Efficacy of IV TXA in Reducing Blood Loss After Elective C-section: Prospective, Randomized, Double-blind, Placebo Controlled
PREVENTION ANEMIA Oral iron IV iron gluconate (order set #233) TRANSEXAMIC ACID Efficacy of IV TXA in Reducing Blood Loss After Elective C-section: Prospective, Randomized, Double-blind, Placebo Controlled
Hematology Emergencies: Problems with Platelets
 Hematology Emergencies: Problems with Platelets Christian Cable, MD, FACP Associate Professor of Medicine Division of Hematology & Oncology Texas A&M HSC College of Medicine Scott & White Healthcare Fundamentals
Hematology Emergencies: Problems with Platelets Christian Cable, MD, FACP Associate Professor of Medicine Division of Hematology & Oncology Texas A&M HSC College of Medicine Scott & White Healthcare Fundamentals
10/8/2013. Drug-induced immune thrombocytopenia (DITP) Clinical aspects
 Clinical aspects") Richard Aster, MD Blood Center of Wisconsin, Blood Research Institute, Milwaukee, WI Senior Investigator Medical College of Wisconsin Professor, Departments of Medicine & Pathology Drug-induced immune
Richard Aster, MD Blood Center of Wisconsin, Blood Research Institute, Milwaukee, WI Senior Investigator Medical College of Wisconsin Professor, Departments of Medicine & Pathology Drug-induced immune
Blood essentials. 16 Nursing made Incredibly Easy! March/April 2013
 Blood essentials One unit of whole blood yields many components that are used to support life-threatening conditions. Managing blood transfusions requires knowledge of blood products and practice guidelines
Blood essentials One unit of whole blood yields many components that are used to support life-threatening conditions. Managing blood transfusions requires knowledge of blood products and practice guidelines
STANDARD BLOOD PRODUCTS AND SERVICES
 STANDARD BLOOD PRODUCTS AND SERVICES Policy NHP reimburses contracted providers for the medically necessary administration (transfusion) of blood and standard blood products. Prerequisites Authorization,
STANDARD BLOOD PRODUCTS AND SERVICES Policy NHP reimburses contracted providers for the medically necessary administration (transfusion) of blood and standard blood products. Prerequisites Authorization,
Aim. To provide basic knowledge on the processing, testing and issue of blood donations by NHSBT
 From Donor To Door Aim To provide basic knowledge on the processing, testing and issue of blood donations by NHSBT At the end of this session you will be aware of: The stages of processing, testing and
From Donor To Door Aim To provide basic knowledge on the processing, testing and issue of blood donations by NHSBT At the end of this session you will be aware of: The stages of processing, testing and
Cardiovascular (connective tissue)
") Cardiovascular (connective tissue) Blood Connective tissue Blood Proteins 7% Plasma 55% Other solutes 2% Water 91% Erythrocytes ~5.2 million per cubic mm Formed elements 45% Leukocytes ~7 thousand per
Cardiovascular (connective tissue) Blood Connective tissue Blood Proteins 7% Plasma 55% Other solutes 2% Water 91% Erythrocytes ~5.2 million per cubic mm Formed elements 45% Leukocytes ~7 thousand per
Primary hemostasis. Vascular endothelium Vasoconstriction : local tissue factor, nervous system
 Primary hemostasis Vascular endothelium Vasoconstriction : local tissue factor, nervous system Platelet Plug Platelet Adhesion Platelet Activation Platelet Aggregation Platelet Plug Formation Secondary
Primary hemostasis Vascular endothelium Vasoconstriction : local tissue factor, nervous system Platelet Plug Platelet Adhesion Platelet Activation Platelet Aggregation Platelet Plug Formation Secondary
Hemostasis/Thrombosis IV
 Hemostasis/Thrombosis IV Antithrombotic Therapy Antithrombotic Therapy Mainstay of battle against thromboembolic disease Hot area of new drug research Cannot inhibit clot formation without increased risk
Hemostasis/Thrombosis IV Antithrombotic Therapy Antithrombotic Therapy Mainstay of battle against thromboembolic disease Hot area of new drug research Cannot inhibit clot formation without increased risk
بسم اهلل الرمحن الرحيم
 بسم اهلل الرمحن الرحيم Definition Multiple myeloma is a neoplastic plasma cell dyscrasia (PCD) that generally produced a monoclonal immunoglobulin protein, characterized by a clinical pentad: (a) anemia;
بسم اهلل الرمحن الرحيم Definition Multiple myeloma is a neoplastic plasma cell dyscrasia (PCD) that generally produced a monoclonal immunoglobulin protein, characterized by a clinical pentad: (a) anemia;
Home truths... the clinical use of components in the UK. Jonathan Wallis. Platelets, FFP, Cryoprecipitate
 Home truths... the clinical use of components in the UK Platelets, FFP, Cryoprecipitate Jonathan Wallis Mar-01 Mar-02 Mar-03 Mar-04 Mar-05 Mar-06 Mar-07 Mar-08 Mar-09 Mar-10 Mar-11 Mar-12 E&N.Wales Platelet
Home truths... the clinical use of components in the UK Platelets, FFP, Cryoprecipitate Jonathan Wallis Mar-01 Mar-02 Mar-03 Mar-04 Mar-05 Mar-06 Mar-07 Mar-08 Mar-09 Mar-10 Mar-11 Mar-12 E&N.Wales Platelet
Veins Valves prevent engorgement and backflow. Baroreceptor reflex. Veins returning blood
 Veins have large radii and low resistance. Walls are thin, not elastic Most blood volume is in veins Veins returning blood Veins Valves prevent engorgement and backflow Sympathetic NS constricts veins
Veins have large radii and low resistance. Walls are thin, not elastic Most blood volume is in veins Veins returning blood Veins Valves prevent engorgement and backflow Sympathetic NS constricts veins
Neupogen. Neupogen (filgrastim) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.10 Subject: Neupogen Page: 1 of 7 Last Review Date: September 15, 2017 Neupogen Description Neupogen
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.10 Subject: Neupogen Page: 1 of 7 Last Review Date: September 15, 2017 Neupogen Description Neupogen
10/17/ /17/2017
 Apheresis Objectives: Explain the concept of cell centrifugation Explain the concept of extracorporeal volume Name 2 methods of venous access for apheresis 1 What is Apheresis? Elements: Whole blood removal
Apheresis Objectives: Explain the concept of cell centrifugation Explain the concept of extracorporeal volume Name 2 methods of venous access for apheresis 1 What is Apheresis? Elements: Whole blood removal
Veins Valves prevent engorgement and backflow. Baroreceptor reflex. Veins returning blood
 Veins have large radii and low resistance. Walls are thin, not elastic Most blood volume is in veins Veins returning blood Veins Valves prevent engorgement and backflow Sympathetic NS constricts veins
Veins have large radii and low resistance. Walls are thin, not elastic Most blood volume is in veins Veins returning blood Veins Valves prevent engorgement and backflow Sympathetic NS constricts veins
LABORATORY APPROACH TO BLEEDING DISORDERS DR NISHANTH PG 1 ST YEAR DEPARTMENT OF PATHOLOGY
 LABORATORY APPROACH TO BLEEDING DISORDERS DR NISHANTH PG 1 ST YEAR DEPARTMENT OF PATHOLOGY 1 WHEN IS THE LAB REQUIRED TO INVESTIGATE FOR A POSSIBLE BLEEDING DISORDER? Clinically suspected bleeding tendency
LABORATORY APPROACH TO BLEEDING DISORDERS DR NISHANTH PG 1 ST YEAR DEPARTMENT OF PATHOLOGY 1 WHEN IS THE LAB REQUIRED TO INVESTIGATE FOR A POSSIBLE BLEEDING DISORDER? Clinically suspected bleeding tendency
Quality Parameters of Platelet Concentrate at Kenyatta National Hospital s Blood Transfusion Unit
 International Journal of Hematological Disorders, 2014, Vol. 1, No. 1, 35-40 Available online at http://pubs.sciepub.com/ijhd/1/1/7 Science and Education Publishing DOI:10.12691/ijhd-1-1-7 Quality Parameters
International Journal of Hematological Disorders, 2014, Vol. 1, No. 1, 35-40 Available online at http://pubs.sciepub.com/ijhd/1/1/7 Science and Education Publishing DOI:10.12691/ijhd-1-1-7 Quality Parameters
Neulasta Fulphila. Neulasta (pegfilgrastim), Fulphila (pegfilgrastim-jmdb) Description
, Fulphila (pegfilgrastim-jmdb) Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.09 Subject: Neulasta Fulphila Page: 1 of 5 Last Review Date: September 20, 2018 Neulasta Fulphila
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.09 Subject: Neulasta Fulphila Page: 1 of 5 Last Review Date: September 20, 2018 Neulasta Fulphila
Virtual Lectures Planning Committee Disclosure Summary
 VIRTUAL LECTURES Cold-Stored Whole Blood and Cold-Stored Platelets MFMER Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo
VIRTUAL LECTURES Cold-Stored Whole Blood and Cold-Stored Platelets MFMER Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo
Bivalirudin (Angiomax ) vs. Heparin during Peripheral Vascular Interventions: Which is Better and How to Decide?
 vs. Heparin during Peripheral Vascular Interventions: Which is Better and How to Decide?") Bivalirudin (Angiomax ) vs. Heparin during Peripheral Vascular Interventions: Which is Better and How to Decide? Vinod Nair MD FACC FSCAI Cardiovascular Ins6tute of the South, Houma Financial Disclosure:
Bivalirudin (Angiomax ) vs. Heparin during Peripheral Vascular Interventions: Which is Better and How to Decide? Vinod Nair MD FACC FSCAI Cardiovascular Ins6tute of the South, Houma Financial Disclosure:
ASSESSING THE EFFICACY AND SAFETY OF NORMAL INTRAVENOUS IMMUNOGLOBULIN PRODUCTS FOR MARKETING AUTHORISATIONS
 ASSESSING THE EFFICACY AND SAFETY OF NORMAL INTRAVENOUS IMMUNOGLOBULIN PRODUCTS FOR MARKETING AUTHORISATIONS Guideline Title Assessing the Efficacy and Safety of Normal Intravenous Immunoglobulin Products
ASSESSING THE EFFICACY AND SAFETY OF NORMAL INTRAVENOUS IMMUNOGLOBULIN PRODUCTS FOR MARKETING AUTHORISATIONS Guideline Title Assessing the Efficacy and Safety of Normal Intravenous Immunoglobulin Products
Congenital Fibrinogen Deficiency. Claude Negrier, MD, PhD Hôpital Louis Pradel Université Claude Bernard Lyon 1
 Congenital Fibrinogen Deficiency Claude Negrier, MD, PhD Hôpital Louis Pradel Université Claude Bernard Lyon 1 claude.negrier@chu-lyon.fr Afibrinogenaemia Clinical presentation Phenotypic and genotypic
Congenital Fibrinogen Deficiency Claude Negrier, MD, PhD Hôpital Louis Pradel Université Claude Bernard Lyon 1 claude.negrier@chu-lyon.fr Afibrinogenaemia Clinical presentation Phenotypic and genotypic
Prior Authorization Criteria Hemophilia/Blood Factor Products
 Prior Authorization Criteria Hemophilia/Blood Factor Products All requests for Hemophilia/Blood Factor Products require a prior authorization and will be screened for medical necessity and appropriateness
Prior Authorization Criteria Hemophilia/Blood Factor Products All requests for Hemophilia/Blood Factor Products require a prior authorization and will be screened for medical necessity and appropriateness
Medical Issues in a Clinical Cellular Therapy Laboratory. Kala Mohandas, MD Director, Cellular Therapy Lab Montefiore Medical Center Bronx, NY
 Medical Issues in a Clinical Cellular Therapy Laboratory Kala Mohandas, MD Director, Cellular Therapy Lab Montefiore Medical Center Bronx, NY Objectives Major, Minor and Bidirectional ABO Incompatibility
Medical Issues in a Clinical Cellular Therapy Laboratory Kala Mohandas, MD Director, Cellular Therapy Lab Montefiore Medical Center Bronx, NY Objectives Major, Minor and Bidirectional ABO Incompatibility
Platelet Factor IV- Heparin Antibodies. Presenter: Michael J. Warhol, M.D.
 Platelet Factor IV- Heparin Antibodies Presenter: Michael J. Warhol, M.D. Learning Objectives Describe the mechanism of interaction between Heparin and Platelet Factor 4 Review the chemistry of Heparin
Platelet Factor IV- Heparin Antibodies Presenter: Michael J. Warhol, M.D. Learning Objectives Describe the mechanism of interaction between Heparin and Platelet Factor 4 Review the chemistry of Heparin
APHERESIS PLATELETS POTENTIAL ADVANTAGES 9/14/2015. Platelet Components. Petteway-Shepherd Award Recipients NCABB Present
 CONTINUING CONTROVERSIES IN PLATELET TRANSFUSION THERAPY Paul M. Ness, M.D. Professor Pathology, Medicine, and Oncology The Johns Hopkins Medical Institutions Baltimore, Maryland, USA Petteway-Shepherd
CONTINUING CONTROVERSIES IN PLATELET TRANSFUSION THERAPY Paul M. Ness, M.D. Professor Pathology, Medicine, and Oncology The Johns Hopkins Medical Institutions Baltimore, Maryland, USA Petteway-Shepherd
Component Preparation, Manufacturing and Modifications
 Component Preparation, Manufacturing and Modifications Mahdokht Parsi, MPH, MT(ASCP) Director of Operation, Immunohematology & Genomics Mparsi@nybc.org Current Practices in Transfusion Medicine 1 NEW YORK
Component Preparation, Manufacturing and Modifications Mahdokht Parsi, MPH, MT(ASCP) Director of Operation, Immunohematology & Genomics Mparsi@nybc.org Current Practices in Transfusion Medicine 1 NEW YORK
Hemostasis and Thrombosis
 Hemostasis Hemostasis and Thrombosis Normal hemostasis is a consequence of tightly regulated processes that maintain blood in a fluid state in normal vessels, yet also permit the rapid formation of a hemostatic
Hemostasis Hemostasis and Thrombosis Normal hemostasis is a consequence of tightly regulated processes that maintain blood in a fluid state in normal vessels, yet also permit the rapid formation of a hemostatic
What Can We Learn from Animal Models of Coagulopathy and Bleeding (about plasma transfusion)?
?") Test What Can We Learn from Animal Models of Coagulopathy and Bleeding (about plasma transfusion)? William Sheffield Associate Director, Research CBS Centre for Innovation, and Professor, Pathology and
Test What Can We Learn from Animal Models of Coagulopathy and Bleeding (about plasma transfusion)? William Sheffield Associate Director, Research CBS Centre for Innovation, and Professor, Pathology and
New York State Council on Human Blood and Transfusion Services
 New York State Council on Human Blood and Transfusion Services GUIDELINES FOR THE ADMINISTRATION OF PLATELETS Second Edition 2006 New York State Council on Human Blood and Transfusion Services New York
New York State Council on Human Blood and Transfusion Services GUIDELINES FOR THE ADMINISTRATION OF PLATELETS Second Edition 2006 New York State Council on Human Blood and Transfusion Services New York
Life Blood. Issue 22. Index. t: medical website clinical guidelines products & services. Dear Life Blood Reader <---

O NO YOU DIDN T! AN ABO-MISMATCHED PLATELET TRANSFUSION
 O NO YOU DIDN T! AN ABO-MISMATCHED PLATELET TRANSFUSION L A U R I E W O L F M L S ( A S C P ) S B B U N I V E R S I T Y O F K A N S A S H O S P I T A L PATIENT OVERVIEW 11-4-2011 56 y/o male with a history
O NO YOU DIDN T! AN ABO-MISMATCHED PLATELET TRANSFUSION L A U R I E W O L F M L S ( A S C P ) S B B U N I V E R S I T Y O F K A N S A S H O S P I T A L PATIENT OVERVIEW 11-4-2011 56 y/o male with a history
Pharmacology Lecture 5. Anticoagulants
 Pharmacology Lecture 5 Anticoagulants General overview Anti-thrombotic Drugs Antiplatlets Anticoagulants Fibrinolytics Anticoagulants Indirect Thrombin Inhibitors Anti-thrombotic effect is exerted by interaction
Pharmacology Lecture 5 Anticoagulants General overview Anti-thrombotic Drugs Antiplatlets Anticoagulants Fibrinolytics Anticoagulants Indirect Thrombin Inhibitors Anti-thrombotic effect is exerted by interaction
Studies on components of. Blood and its functions
 Chapter 2 An introduction to blood groups and blood transfusion in domestic animals Aasif Ahmad Sheikh 1 *; Showkat Ahmad Bhat 2 ; Ankita Kalyan 1 ; Mohammad Rayees Dar 1 1 Animal Physiology Division,
Chapter 2 An introduction to blood groups and blood transfusion in domestic animals Aasif Ahmad Sheikh 1 *; Showkat Ahmad Bhat 2 ; Ankita Kalyan 1 ; Mohammad Rayees Dar 1 1 Animal Physiology Division,
6TH EDITION OF FACT-JACIE STANDARDS A QUICK SUMMARY. BHS JACIE Day, 6 March 2015 Eoin McGrath JACIE Operations Manager
 6TH EDITION OF FACT-JACIE STANDARDS A QUICK SUMMARY BHS JACIE Day, 6 March 2015 Eoin McGrath JACIE Operations Manager CONTENTS Review process Sources of information Selection of main changes and developments
6TH EDITION OF FACT-JACIE STANDARDS A QUICK SUMMARY BHS JACIE Day, 6 March 2015 Eoin McGrath JACIE Operations Manager CONTENTS Review process Sources of information Selection of main changes and developments
Ain t Nobody Got Time for
 Ain t Nobody Got Time for DATs Lindsay Peters MLS(ASCP)SBB Reference Laboratory Supervisor Mississippi Valley Regional Blood Center OBJECTIVES Define and describe the antiglobulin test. Identify the reagents
Ain t Nobody Got Time for DATs Lindsay Peters MLS(ASCP)SBB Reference Laboratory Supervisor Mississippi Valley Regional Blood Center OBJECTIVES Define and describe the antiglobulin test. Identify the reagents
Apheresis M. Flores, BSN, RN, HP (ASCP)
") Apheresis M. Flores, BSN, RN, HP (ASCP) Objectives: 1. Discuss Apheresis and key concepts 2. Discuss : Cell Collection Extracorporeal Photopheresis (ECP) 1 What is Apheresis? Apheresis: Greek word meaning
Apheresis M. Flores, BSN, RN, HP (ASCP) Objectives: 1. Discuss Apheresis and key concepts 2. Discuss : Cell Collection Extracorporeal Photopheresis (ECP) 1 What is Apheresis? Apheresis: Greek word meaning
EDUCATIONAL COMMENTARY MASSIVE TRANSFUSION PROTOCOL
 EDUCATIONAL COMMENTARY MASSIVE TRANSFUSION PROTOCOL Commentary provided by: Kathleen Trudell MLS (ASCP) CM SBBCM University of Nebraska Medical Center Division of Medical Laboratory Science College of
EDUCATIONAL COMMENTARY MASSIVE TRANSFUSION PROTOCOL Commentary provided by: Kathleen Trudell MLS (ASCP) CM SBBCM University of Nebraska Medical Center Division of Medical Laboratory Science College of
Microparticles in platelet concentrates are a key indicator of the level of platelet activation. This is a topic that is critically important to
 Microparticles in platelet concentrates are a key indicator of the level of platelet activation. This is a topic that is critically important to understand in more detail. Based on the literature between
Microparticles in platelet concentrates are a key indicator of the level of platelet activation. This is a topic that is critically important to understand in more detail. Based on the literature between
Princess Alexandra Hospital Emergency Department. Clinical Procedure. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Procedure Trauma, Resuscitation Review Officer: Glenn Ryan 1 Introduction Version no: 1 Approval Date: 16/07/2014 Review Date: 16/07/2016 Authority:
Princess Alexandra Hospital Emergency Department Clinical Procedure Trauma, Resuscitation Review Officer: Glenn Ryan 1 Introduction Version no: 1 Approval Date: 16/07/2014 Review Date: 16/07/2016 Authority:
chronic leukemia lymphoma myeloma differentiated 14 September 1999 Transformed Pre- Ig Surface Surface Secreted B- ALL Macroglobulinemia Myeloma
 Disease Usual phenotype acute leukemia precursor chronic leukemia lymphoma myeloma differentiated Pre- B-cell B-cell Transformed B-cell Plasma cell Ig Surface Surface Secreted Major malignant counterpart
Disease Usual phenotype acute leukemia precursor chronic leukemia lymphoma myeloma differentiated Pre- B-cell B-cell Transformed B-cell Plasma cell Ig Surface Surface Secreted Major malignant counterpart
Disclosure. Hemophilia: The Royal Treatment. Objectives. Background. History of Hemophilia. Epidemiology 1/4/2018
 Disclosure Hemophilia: The Royal Treatment Nikki Heeren, PharmD PGY1 Resident Avera McKennan Hospital I have had no financial relationship over the past 12 months with any commercial sponsor with a vested
Disclosure Hemophilia: The Royal Treatment Nikki Heeren, PharmD PGY1 Resident Avera McKennan Hospital I have had no financial relationship over the past 12 months with any commercial sponsor with a vested
Clinical Procedure. ROTEM Trauma, Resuscitation. Princess Alexandra Hospital Emergency Department. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Procedure Trauma, Resuscitation Review Officer: Glenn Ryan 1 Introduction Version no: 1 Approval Date: 16/07/2014 Review Date: 16/07/2016 Authority:
Princess Alexandra Hospital Emergency Department Clinical Procedure Trauma, Resuscitation Review Officer: Glenn Ryan 1 Introduction Version no: 1 Approval Date: 16/07/2014 Review Date: 16/07/2016 Authority:
An Unusual Presentation in a Man of Advanced Age. Robert E. Richard
 An Unusual Presentation in a Man of Advanced Age Robert E. Richard An Unusual Presentation by a Man of Advanced Age Robert E. Richard A few observations on what ht makes aesaa good fellows eo sconference
An Unusual Presentation in a Man of Advanced Age Robert E. Richard An Unusual Presentation by a Man of Advanced Age Robert E. Richard A few observations on what ht makes aesaa good fellows eo sconference
Surgical Adhesives in Facial Plastic Surgery
 Surgical Adhesives in Facial Plastic Surgery Dean M. Toriumi, Victor K. Chung, Quintin M. Cappelle University of Illinois at Chicago Chicago, IL Supplement to Toriumi DM, Chung VK, Cappelle QM. Surgical
Surgical Adhesives in Facial Plastic Surgery Dean M. Toriumi, Victor K. Chung, Quintin M. Cappelle University of Illinois at Chicago Chicago, IL Supplement to Toriumi DM, Chung VK, Cappelle QM. Surgical
POST-ISTH: Novità dal meeting di Toronto 2015 Piastrine: fisiopatologia. Erica De Candia Università Cattolica -Roma
 POST-ISTH: Novità dal meeting di Toronto 2015 Piastrine: fisiopatologia Erica De Candia Università Cattolica -Roma Novità ISTH 2015: Piastrine: Fisiopatologia i) Alternative platelet function throughout
POST-ISTH: Novità dal meeting di Toronto 2015 Piastrine: fisiopatologia Erica De Candia Università Cattolica -Roma Novità ISTH 2015: Piastrine: Fisiopatologia i) Alternative platelet function throughout
2111: ALL Post-HCT. Add/ Remove/ Modify. Manual Section. Date. Description. Comprehensive Disease- Specific Manuals
 2111: ALL Post-HCT The Acute Lymphoblastic Leukemia Post-HCT Data Form is one of the Comprehensive Report Forms. This form captures ALL-specific post-hct data such as: planned treatments post-hct, the
2111: ALL Post-HCT The Acute Lymphoblastic Leukemia Post-HCT Data Form is one of the Comprehensive Report Forms. This form captures ALL-specific post-hct data such as: planned treatments post-hct, the
Sign up to receive ATOTW weekly
 RECOMBINANT HUMAN ACTIVATED PROTEIN C IN THE TREATMENT OF SEVERE SEPSIS ANAESTHESIA TUTORIAL OF THE WEEK 133 11 TH MAY 2009 Dr Richard Eve, Royal Cornwall Hospital, Cornwall, UK Correspondence to richardlloydeve@gmail.com
RECOMBINANT HUMAN ACTIVATED PROTEIN C IN THE TREATMENT OF SEVERE SEPSIS ANAESTHESIA TUTORIAL OF THE WEEK 133 11 TH MAY 2009 Dr Richard Eve, Royal Cornwall Hospital, Cornwall, UK Correspondence to richardlloydeve@gmail.com
Transfus Med Hemother 2009;36:
 Transfus Med Hemother 2009;36:419 436 7 Procoagulators 7.1 Fibrinogen 7.1.1 Preparation, Quality Criteria 7.1.2 Active Constituents 7.1.3 Physiological Function 7.1.4 Application 7.1.4.1 Congenital Fibrinogen
Transfus Med Hemother 2009;36:419 436 7 Procoagulators 7.1 Fibrinogen 7.1.1 Preparation, Quality Criteria 7.1.2 Active Constituents 7.1.3 Physiological Function 7.1.4 Application 7.1.4.1 Congenital Fibrinogen
Haemostasis. The function of haemostasis is: to prevent blood loss from injured vessels. to stop bleeding. to prevent thrombosis
 Haemostasis Haemostasis The function of haemostasis is: to prevent blood loss from injured vessels to stop bleeding to prevent thrombosis Haemostasis blood endothelium basement membrane subendothelium
Haemostasis Haemostasis The function of haemostasis is: to prevent blood loss from injured vessels to stop bleeding to prevent thrombosis Haemostasis blood endothelium basement membrane subendothelium
The Cat s Out of the Bag: Microbiological Investigations of Acute Transfusion Reactions.
 The Cat s Out of the Bag: Microbiological Investigations of Acute Transfusion Reactions. Philippe Lagacé-Wiens, MD FRCPC, DTM&H plagacewiens@sharedhealthmb.ca COI declaration I have no conflicts, real
The Cat s Out of the Bag: Microbiological Investigations of Acute Transfusion Reactions. Philippe Lagacé-Wiens, MD FRCPC, DTM&H plagacewiens@sharedhealthmb.ca COI declaration I have no conflicts, real
Mouse von Willebrand Factor (vwf) ELISA Kit
 ELISA Kit") Mouse von Willebrand Factor (vwf) ELISA Kit Catalog No. CSB-E08439m (96T) This immunoassay kit allows for the in vitro quantitative determination of mouse vwf concentrations in cell culture supernates,
Mouse von Willebrand Factor (vwf) ELISA Kit Catalog No. CSB-E08439m (96T) This immunoassay kit allows for the in vitro quantitative determination of mouse vwf concentrations in cell culture supernates,
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency Evaluation of Medicines for Human Use London, 29 July 2004 CPMP/BPWG/1089/00 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON THE CLINICAL INVESTIGATION OF PLASMA
European Medicines Agency Evaluation of Medicines for Human Use London, 29 July 2004 CPMP/BPWG/1089/00 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) GUIDELINE ON THE CLINICAL INVESTIGATION OF PLASMA