Beta interferon and glatiramer acetate for treating multiple sclerosis (review of TA32)
|
|
|
- Laurel Caldwell
- 5 years ago
- Views:
Transcription
1 Public slides part 1 (Redacted) Beta interferon and glatiramer acetate for treating multiple sclerosis (review of TA32) 3 rd Appraisal Committee meeting Committee B, 16 th November 2017 Previous Appraisal Committee meetings November 2016 and May 2017 Companies: Bayer, Biogen, Merck Serono, Novartis, Teva Chair: Amanda Adler Assessment group: Warwick Evidence NICE technical team: Thomas Palmer, Jasdeep Hayre 1
2 Key issues Which effectiveness estimate from the Risk Sharing Scheme should be used in the economic model? Which approach to modelling MS-related mortality risk does the committee prefer? For clinically isolated syndrome, are beta interferons and glatiramer acetate relevant in the treatment pathway? 2
3 History of this appraisal and NICE guidance Previous Appraisal Current Appraisal 1. Beta interferon Rebif Avonex Betaferon 2. Glatiramer acetate TA32 (2002): Not recommended New products 1. Beta interferon Interferon 1b (Extavia) Pegylated interferon beta 1a (Plegridy) 2. Glatiramer acetate New formulation (Copaxone) DoH Risk sharing scheme (RSS) Data collection on clinical outcomes 1 st and 2 nd meetings Long term outcome data from Risk Sharing Scheme available Appraisal suspended pending additional work No ACD issued RSS ended rd meeting TODAY Patient access schemes for Rebif and Extavia New analyses 3
4 Multiple sclerosis Clinically isolated syndrome - CIS 1 st clinical episode with features of MS May not develop into clinically definite MS Relapsing-remitting MS (RRMS) Clearly defined relapses 3 groups based on NICE guidance: 1. RRMS 2. Highly active 3. Rapidly evolving 85-90% of people at diagnosis Secondary progressive MS Some patients continue to have relapses so may continue disease modifying therapies ~50% within 10 years Glatiramer acetate, IFN β-1a* and IFN β- 1b indicated for CIS All drugs indicated for RRMS *pegifn β-1a not indicated for CIS 4
5 Technologies Summary IFN β-1a pegifn β-1a IFN β-1b Glatiramer Avonex Rebif Plegridy Betaferon Extavia Copaxone RRMS CIS Dose 30 mcg 44 or 22 mcg 125 mcg 250 mcg 250 mcg 20 mg or 40mg Admin IM SC SC SC SC SC Frequency Weekly 3x/week Every 2 weeks Every other day Every other day Daily or 3x/week List cost annual 8,502 7,976 or 10, ,264 6,681-6,704 Discount? RRMS: Relapsing-remitting multiple sclerosis; SPMS: secondary progressive multiple sclerosis; CIS: clinically isolated syndrome; IM: intramuscular; SC: subcutaneous; IFN: interferon 5
6 RRMS: Risk Sharing Scheme (RSS) In original appraisal (TA32), technologies not cost-effective over a 20 year time horizon Treatment effects based on trials with median follow-up ~2 years leading to uncertainty Department of Health (DoH) set up risk-sharing scheme to: provide interferon β-1a (Avonex, Rebif), interferon β-1b (Betaferon) and glatiramer (Copaxone) monitor whether treatments as effective as observed in trials if observed benefits of treatment worse than expected from trials, then price should fall Risk Sharing Scheme does NOT have a control group representing best supportive care British Columbia Multiple Sclerosis cohort used as historical comparator Eligible NHS patients included anyone with relapsing remitting MS (or secondary progressive MS) who continued to relapse and who meet criteria from Association of British Neurologists Confidential discounts and infrastructure contributions 6
7 RRMS: Clinical effectiveness evidence Source Data from Clinical trials ACM1 committee conclusion Key outcomes Network meta-analyses of trials carried out by Assessment Group, Biogen, Merck and Teva Confirmed disability progression Annualised Relapse Rate (ARR) Summary Point estimates broadly similar from each network metaanalysis All drugs slowed disability progression and fewer relapses compared with placebo Results comparing treatments with each other less conclusive Data from Risk Sharing Scheme Department of Health Summary measure of disease progression (i.e. change relative to baseline of a weighted sum of proportions of patients who progressed to each score; weighting factors = loss of utility in each ) All drugs slowed disability progression compared with best supportive care in historical cohort Results for individual drugs are commercial in confidence 7
8 Issue Comparator Clinical trials: RRMS Clinical trials: CIS Relapse rates Disability progression Risk sharing scheme Implied hazard ratio Treatment Waning Committee conclusion from Nov 2016 & May 2017 meetings Most appropriate comparator was best supportive care Possible bias: difference in design, follow-up, insufficient blinding Generalisable and relevant to consider All technologies delayed onset of MS vs placebo Many CIS trials before changes to definition in 2010 Not generalisable for this appraisal All technologies reduced number of relapses vs placebo All technologies had similar effectiveness when compared with best supportive care All technologies delayed progression vs placebo All technologies had similar effectiveness when compared with best supportive care Preferred results from RSS as long follow-up and large number of patients (~xxx patients, mean follow-up: xxx years) More likely to reflect reflected people treated in NHS practice Represents relative effectiveness in slowing disease progression as seen in the RSS, when compared with that expected from people in British Columbia MS cohort on best supportive care Efficacy unlikely to remain constant over time 8
9 Economic models 1 st meeting 2 nd meeting RRMS Risk Sharing Scheme Model with RSS data Same Structure Assessment Group s model Teva Biogen Merck Similar structures but different data Assessment Group s model Committee preferred assumptions CIS Assessment Group s model Merck s model Assessment Group s model Different structures and data 9
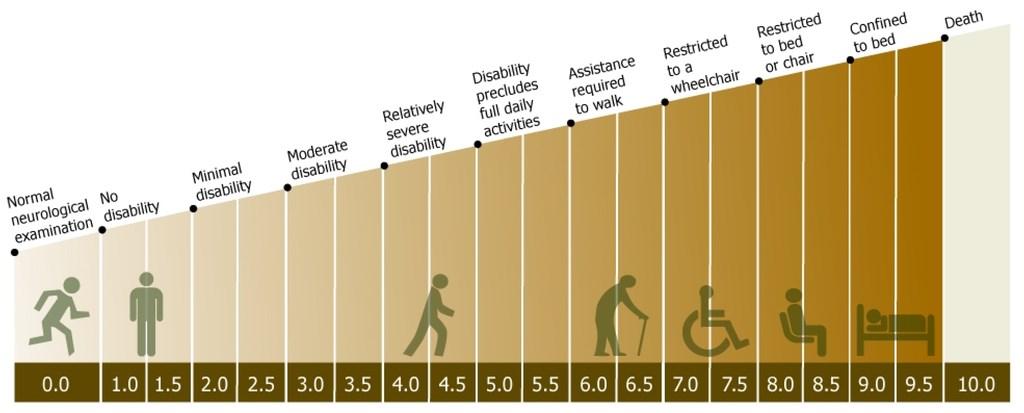
10 Expanded Disability Status Scale () 10
11 RRMS: Risk Sharing Scheme Model Relapsing-remitting MS Death Secondary progressive MS Cycled yearly Starting age 30 years Can die from MS only in 7-9 Model Assumptions 50-year time horizon Natural history of RRMS (best supportive care) based on British Columbia MS cohort (n=898) 11
12 How treatments increase QALYs in RRMS model Increased qualityadjusted life years Improved quality of life Length of life Slower disability progression, more time spent in lower states Fewer relapses Reduced caregiver disutility Very little difference between treatments 12
13 Risk Sharing Scheme model: effectiveness inputs Parameter Value Source Proportion of people who stop treatment each year 5% Risk Sharing Scheme data Annual relapse rate RR (95% CI) 0.72 (CI not reported) MS Trust Survey 2002 Implied Progression 0.79 (0.77, 0.81) Risk Sharing Scheme data HR (95% CI) CI: confidence interval, HR: hazard ratio, RR: rate ratio Risk Sharing Scheme pooled results for all treatments Combined treatment effect of: IFN β-1a 44 or 22 mcg SC 3 times a week (Rebif) GA 20 mg SC daily (Copaxone) IFN β-1b 250 mcg SC every other day (Betaferon) IFN β-1a 30 mcg IM weekly (Avonex) Assessment Group: used RSS data in its base case RSS estimate more robust : Network meta-analysis of trial has limited sample size & follow-up: may overestimate effects of treatment 13
14 Effectiveness of individual drugs vs pooled drugs RSS data (used by Assessment Group for modelling) for pooled and individual effectiveness of treatments are not directly comparable Pooled analysis uses all available data are used, including data after patients switch to another treatment Individual data excludes data after patients switch to another treatment Possible source of bias, as patients who switch DMTs are likely to have experienced either worse disease progression or worse side effects Using pooled effectiveness estimates that are more comparable with individual effectiveness estimates (i.e. C1b below) would lower ICERs in the pooled analysis Variant Assumptions Implied hazard ratio Base-case All data C1a Excluding data after patients switch to a disease modifying therapy that wasn t in RSS C1b Excluding data after patients switch to any other disease modifying therapy Which effectiveness estimate is appropriate for the economic model? 14
15 Results of cost effectiveness Not provided in public (but in part 2) because of confidential information about: Effectiveness from Risk Sharing Scheme Confidential discounts Updated from 2 nd committee meeting (May 2017): New patient access schemes for Extavia and Rebif New assumption about mortality proposed by Merck health state costs adjusted for inflation to 2015/16 levels 15
16 Issues Natural history Effectiveness for RRMS Effectiveness for CIS Treatment waning Committee preferred modelling assumptions (Nov 2016 and May 2017 meetings) Preferred British Columbia MS database Pooled RSS effectiveness data for all treatments (including Plegridy, which was not part of the RSS) Network of trials until diagnosis of MS & data from Risk Sharing Scheme for RRMS stage Assume treatment waning (i.e. 50% reduction in effectiveness after year 10 of treatment) Backward transitions Assume that interferon & glatiramer acetate do not impact on backward transition (people don't improve to less severe health states) Discontinuation from Use RSS discontinuation rates (i.e. 5% discontinue treatment treatment every year) Prices for drugs Use only list prices, Commercial Medicines Unit agreements or Patient Access Scheme discounts Utilities Include carers disutilities health state Preferred UK MS Survey health state costs costs Analysis Pairwise vs best supportive care 16
17 Further evidence after May 2017 committee meeting Some companies indicated that they were considering access agreements for their technologies, which meant that the basis for decision making was likely to change. NICE shared the main committee conclusions with the companies. In response NICE received: New submissions from: Biogen (Avonex, Plegridy) Merck (Rebif) Teva (Copaxone) New patient access schemes from: Merck (Rebif) Novartis (Extavia) No response from Bayer (Betaferon) 17
18 Biogen (IFN β-1a, Avonex; peg-ifn β-1a, Plegridy) Using RSS data inconsistent with previous appraisals should consider individual treatment data derived from the trial-based network meta-analysis Using RSS for Plegridy and pooling effectiveness when individual treatment results available inappropriate Suggest that model overestimates costs, as the criterion for discontinuing treatment used incorrectly Assessment Group note that this is because of the 1/2-cycle correction applied in the model Assessment Group overestimates treatment waning effect No published evidence to support a waning effect RSS already includes waning inconsistent with previous appraisals Percentage of patients who stop treatment each year lower than other appraisals, with 40% of patients assumed to still be on a DMT after 10 years - does not reflect shift in treatment landscape Assessment group note that the rate is based on empirical data from the RSS, and may be lower due to less active disease in RSS population 18
19 Teva (glatiramer acetate; Copaxone) No scientific justification for assumption of pooled effectiveness to include glatiramer acetate Uncertainty in health state costs has not been adequately addressed Teva suggest using an average of the committee-preferred UK MS Survey costs and the original RSS costs (Kobelt, 2000) Should consider informal care costs, as Teva suggest they have been in previous appraisals (teriflunomide and dimethyl fumarate) Informal care costs were not considered in either of the previous appraisals In those appraisals, the committee explored analyses excluding nonmedical costs because the non-medical costs included informal care costs Unfair and unreasonable that committee has not considered infrastructure contributions (contributions to the NHS) Should inflate health state costs to 2015/16 levels Assessment group have updated the costs used in the new analyses 19
20 Merck (IFN β-1a, Rebif) Provides a new patient access scheme Each product should be assessed using its individual RSS results Merck suggest an alternative to modelling mortality risk Current method: the assessment group assume that MSrelated mortality is captured in transitions to state 10 and non MS-related mortality is equal to the general population Merck method: Standardised mortality ratio (MS compared to general population) used for levels to capture the increased risk of mortality associated with MS Reflects mortality assumptions in recent MS submissions (TA254, TA303, TA312 and TA441) 20
21 Standardised mortality ratio, SMR Assessment Group s original report highlighted concerns over doublecounting MS-related mortality in the model SMR of 2.0 was applied to general population mortality, in addition to MS-related mortality captured in transitions to state 10 Department of Health: SMR used to capture the increased risk of non- MS related mortality in MS patients Assessment Group changed non-ms related mortality risk to be the same as the general population, as risk of MS-related death captured in transition matrices Little impact on cost-effectiveness An alternative approach to capturing increased risk of mortality for those with MS is using SMRs ( mortality multipliers ) for states below 10 This was implemented in previous appraisals using mortality multipliers from Pokorski (1997): standardised mortality ratio of at 0-3, at 4-6, and at 7-9 Analyses using this assumption now provided by Assessment Group 21
22 Pokorski (1997) mortality multipliers TA441 ERG critique ERG noted that data used in the model, quoted in Pokorski et al 1997, were from a secondary reference: Sadovnick et al (1992) Sadovnick examined mortality (115 deaths) amongst two groups of Canadian MS patients from Ontario and British Columbia (N = 2348) Cases were classified as mild, moderate and severe MS on the basis of scores (0 to 3.5, 4 to 7, 7 respectively) scores were only collected at the first clinical visit, while the actual score at time of death will depend on the speed of progression in the particular population studied ERG expressed concerns that the study did not provide reliable estimates for making comparison with current MS population Improved care and exposure to disease modifying therapies since the study, likely large differences in smoking prevalence and geographical dissimilarities Which mortality assumption does the committee prefer? 22
23 CIS: Clinically isolated syndrome Clinically isolated syndrome refers to first episode of neurological symptoms McDonald criteria for diagnosing multiple sclerosis revised in 2010 Can diagnose MS after a single neurological event with supporting magnetic resonance imaging (MRI) At 1 st committee meeting: heard that CIS patients in trials at high-risk of developing MS ( McDonald MS ) would be treated as MS At 2 nd committee meeting: heard that relevance of CIS continues to decline, with upcoming revisions to diagnostic criteria Assessment Group s network meta-analysis included 5 studies, main outcome: time to conversion to clinically definite MS All treatments delayed the onset of MS compared with placebo Uncertain whether in clinical practice treatment aims to delay onset of MS, and therefore the relevance of these trials is unclear 23
24 CIS: Clinically isolated syndrome clinician comments (1) Due to uncertainty on clinically isolated syndrome (CIS) at the previous committee meeting, NICE contacted 4 clinical experts from recent MSrelated appraisals to ask the following questions: Is CIS still relevant in the clinical pathway for MS? Yes new guidelines released in 2017 may change the situation Ever lesser relevance still a group with CIS but most likely to represent the milder end of spectrum Yes CIS is a holding diagnosis until we can confirm (MS) If so, how often is CIS still diagnosed? About 50% of people are diagnosed as CIS and monitored for the development of MS About 30-40% of patients presenting with their first attack will be CIS Only about 20% of those presenting with a single event will remain having a diagnosis of CIS at 12 months (the rest) will be diagnosed with MS at baseline following investigation or have their diagnosis changed to MS within 6-12 months due to further clinical relapse or new MRI activity 24
25 CIS: Clinically isolated syndrome clinician comments (2) Would treatment for CIS be the same as for first-line treatment for RRMS? We do not usually treat after a single episode Patients remaining as CIS at 12 months are likely to represent a milder group who either may never convert to MS or if they do are unlikely to have relapse frequency to qualify for a MS therapy hence this group will be far less likely to be treated We would not offer them treatments that are licensed for relapsing forms of MS If a patient has CIS and a very active MRI we do treat as RRMS Is a recommendation for treating CIS with disease modifying therapies, separately from treating RRMS, relevant for NHS clinical practice? 25
26 Clinically Isolated Syndrome Adverse events 0 Clinically Isolated Syndrome DMT disease progression Relapsing-remitting MS 1 Best supportive care Assessment Group Model CIS Assumptions 1. Starting population 30 years old 2. No residual benefit from disease modifying therapy (DMT) after progressing to RRMS 3. RRMS pathway same as in RSS model 8 9 disease progression 4. RRMS treatment discontinuation independent of CIS treatment discontinuation DEATH (from any state) 10 Does a model based on disease-modifying therapies delaying the onset of MS for people with CIS reflect clinical practice? 26
27 How treatments increase QALYs in CIS model Clinically isolated syndrome phase: Delayed conversion to multiple sclerosis Increased qualityadjusted life years After conversion to multiple sclerosis, model is the same as for RRMS: Slower disability progression, more time spent in lower states Fewer relapses Reduced caregiver disutility 27
28 Key issues Which effectiveness estimate from the Risk Sharing Scheme should be used in the economic model? Which approach to modelling MS-related mortality risk does the committee prefer? For clinically isolated syndrome, are beta interferons and glatiramer acetate relevant in the treatment pathway? 28
Technology appraisal guidance Published: 22 January 2014 nice.org.uk/guidance/ta303
 Teriflunomide for treating relapsing remitting multiple sclerosis Technology appraisal guidance Published: 22 January 2014 nice.org.uk/guidance/ta303 NICE 2018. All rights reserved. Subject to Notice of
Teriflunomide for treating relapsing remitting multiple sclerosis Technology appraisal guidance Published: 22 January 2014 nice.org.uk/guidance/ta303 NICE 2018. All rights reserved. Subject to Notice of
Technology appraisal guidance Published: 27 August 2014 nice.org.uk/guidance/ta320
 Dimethyl fumarate ate for treating relapsing-remitting multiple sclerosis Technology appraisal guidance Published: 27 August 2014 nice.org.uk/guidance/ta320 NICE 2018. All rights reserved. Subject to Notice
Dimethyl fumarate ate for treating relapsing-remitting multiple sclerosis Technology appraisal guidance Published: 27 August 2014 nice.org.uk/guidance/ta320 NICE 2018. All rights reserved. Subject to Notice
Evidence Review Group s Report Dimethyl fumarate for treating relapsing-remitting multiple sclerosis
 Evidence Review Group s Report Dimethyl fumarate for treating relapsing-remitting multiple sclerosis Produced by CRD and CHE Technology Assessment Group Authors Gill Norman, Research Fellow, CRD Stephen
Evidence Review Group s Report Dimethyl fumarate for treating relapsing-remitting multiple sclerosis Produced by CRD and CHE Technology Assessment Group Authors Gill Norman, Research Fellow, CRD Stephen
Common Drug Review Pharmacoeconomic Review Report
 Common Drug Review Pharmacoeconomic Review Report October 2014 Drug Teriflunomide (Aubagio) (14 mg film-coated tablet) Indication Teriflunomide is indicated as monotherapy for the treatment of patients
Common Drug Review Pharmacoeconomic Review Report October 2014 Drug Teriflunomide (Aubagio) (14 mg film-coated tablet) Indication Teriflunomide is indicated as monotherapy for the treatment of patients
National Horizon Scanning Centre. Cladribine (Movectro) for multiple sclerosis; relapsing-remitting. April 2008
 for multiple sclerosis; relapsing-remitting. April 2008") Cladribine (Movectro) for multiple sclerosis; relapsing-remitting April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not
Cladribine (Movectro) for multiple sclerosis; relapsing-remitting April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not
Evidence Review Group s Report Template This template should be completed with reference to NICEs Guide to the Methods of Single Technology Appraisal
 Evidence Review Group s Report Template This template should be completed with reference to NICEs Guide to the Methods of Single Technology Appraisal Title: Fingolimod for the treatment of relapsing remitting
Evidence Review Group s Report Template This template should be completed with reference to NICEs Guide to the Methods of Single Technology Appraisal Title: Fingolimod for the treatment of relapsing remitting
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Betaseron, Extavia) Reference Number: CP.CPA.331 Effective Date: 06.01.18 Last Review Date: 05.18 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
Clinical Policy: (Betaseron, Extavia) Reference Number: CP.CPA.331 Effective Date: 06.01.18 Last Review Date: 05.18 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Betaseron, Extavia) Reference Number: CP.PHAR.256 Effective Date: 08.01.16 Last Review Date: 05.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at
Clinical Policy: (Betaseron, Extavia) Reference Number: CP.PHAR.256 Effective Date: 08.01.16 Last Review Date: 05.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at
Aubagio (teriflunomide tablets) Policy Number: Last Review: 07/2017 Origination: 07/2014 Next Review: 07/2018
 Policy Number: Last Review: 07/2017 Origination: 07/2014 Next Review: 07/2018") Aubagio (teriflunomide tablets) Policy Number: 5.01.614 Last Review: 07/2017 Origination: 07/2014 Next Review: 07/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Aubagio (teriflunomide tablets) Policy Number: 5.01.614 Last Review: 07/2017 Origination: 07/2014 Next Review: 07/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Alemtuzumab, dimethyl fumarate, laquinimod and teriflunomide for the treatment of relapsing forms of multiple
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Alemtuzumab, dimethyl fumarate, laquinimod and teriflunomide for the treatment of relapsing forms of multiple
There are currently 4 US Food and Drug
 DISEASE-MODIFYING THERAPIES IN RELAPSING-REMITTING MULTIPLE SCLEROSIS* Benjamin M. Greenberg, MD, MHS ABSTRACT Four major disease-modifying therapies are discussed within the context of relapsing and remitting
DISEASE-MODIFYING THERAPIES IN RELAPSING-REMITTING MULTIPLE SCLEROSIS* Benjamin M. Greenberg, MD, MHS ABSTRACT Four major disease-modifying therapies are discussed within the context of relapsing and remitting
HEALTH TECHNOLOGY ASSESSMENT
 HEALTH TECHNOLOGY ASSESSMENT VOLUME 21 ISSUE 52 SEPTEMBER 2017 ISSN 1366-5278 Clinical effectiveness and cost-effectiveness of beta-interferon and glatiramer acetate for treating multiple sclerosis: systematic
HEALTH TECHNOLOGY ASSESSMENT VOLUME 21 ISSUE 52 SEPTEMBER 2017 ISSN 1366-5278 Clinical effectiveness and cost-effectiveness of beta-interferon and glatiramer acetate for treating multiple sclerosis: systematic
National MS Society Information Sourcebook
 National MS Society Information Sourcebook www.nationalmssociety.org/sourcebook Interferons The interferons are a group of natural proteins that are produced by human cells in response to viral infection
National MS Society Information Sourcebook www.nationalmssociety.org/sourcebook Interferons The interferons are a group of natural proteins that are produced by human cells in response to viral infection
Introducing MN-166 Multiple Sclerosis. July 9, 2008
 Introducing MN-166 A New Treatment Paradigm for Multiple Sclerosis July 9, 2008 MediciNova, Inc. 2008 Forward-Looking Statements Statements in this presentation that are not historical in nature constitute
Introducing MN-166 A New Treatment Paradigm for Multiple Sclerosis July 9, 2008 MediciNova, Inc. 2008 Forward-Looking Statements Statements in this presentation that are not historical in nature constitute
A Multiple Treatment Comparison of Eleven Disease- Modifying Drugs Used for Multiple Sclerosis
 Original Article J Clin Med Res. 2018;10(2):88-105 A Multiple Treatment Comparison of Eleven Disease- Modifying Drugs Used for Multiple Sclerosis Vida Hamidi a, Elisabeth Couto a, Tove Ringerike a, Marianne
Original Article J Clin Med Res. 2018;10(2):88-105 A Multiple Treatment Comparison of Eleven Disease- Modifying Drugs Used for Multiple Sclerosis Vida Hamidi a, Elisabeth Couto a, Tove Ringerike a, Marianne
A blood sample will be collected annually for up to 2 years for JCV antibody testing.
 Mellen Center Currently Enrolling Non-Treatment Trials STRATIFY-2 JCV Antibody Program in Patients with Relapsing Multiple Sclerosis Receiving or Considering Treatment with Tysabri Primary Investigator:
Mellen Center Currently Enrolling Non-Treatment Trials STRATIFY-2 JCV Antibody Program in Patients with Relapsing Multiple Sclerosis Receiving or Considering Treatment with Tysabri Primary Investigator:
Multiple Sclerosis Agents
 Multiple Sclerosis Agents Policy Number: 5.01.614 Last Review: 09/2018 Origination: 07/2014 Next Review: 09/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Multiple Sclerosis Agents Policy Number: 5.01.614 Last Review: 09/2018 Origination: 07/2014 Next Review: 09/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
MS Injectable Drugs
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: MS Injectable Drugs Page: 1 of 5 Last Review Date: November 30, 2018 MS Injectable Drugs Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: MS Injectable Drugs Page: 1 of 5 Last Review Date: November 30, 2018 MS Injectable Drugs Description
Disease-Modifying Therapies for Relapsing- Remitting and Primary-Progressive Multiple Sclerosis: Effectiveness and Value
 Disease-Modifying Therapies for Relapsing- Remitting and Primary-Progressive Multiple Sclerosis: Effectiveness and Value Response to Public Comments on Draft Evidence Report January 26, 2017 Institute
Disease-Modifying Therapies for Relapsing- Remitting and Primary-Progressive Multiple Sclerosis: Effectiveness and Value Response to Public Comments on Draft Evidence Report January 26, 2017 Institute
Cost-effectiveness analysis of glatiramer acetate in the treatment of relapsing-remitting multiple sclerosis Bose U, Ladkani D, Burrell A, Sharief M
 Cost-effectiveness analysis of glatiramer acetate in the treatment of relapsing-remitting multiple sclerosis Bose U, Ladkani D, Burrell A, Sharief M Record Status This is a critical abstract of an economic
Cost-effectiveness analysis of glatiramer acetate in the treatment of relapsing-remitting multiple sclerosis Bose U, Ladkani D, Burrell A, Sharief M Record Status This is a critical abstract of an economic
The Cost-Effectiveness of Treatment Options for Relapsing-Remitting and Primary Progressive Multiple Sclerosis: Modeling Analysis Plan
 The Cost-Effectiveness of Treatment Options for Relapsing-Remitting and Primary Progressive Multiple Sclerosis: Modeling Analysis Plan October 7, 2016 Prepared for Institute for Clinical and Economic Review,
The Cost-Effectiveness of Treatment Options for Relapsing-Remitting and Primary Progressive Multiple Sclerosis: Modeling Analysis Plan October 7, 2016 Prepared for Institute for Clinical and Economic Review,
Lemtrada (alemtuzumab)
") Lemtrada (alemtuzumab) Policy Number: 5.02.517 Last Review: 7/2018 Origination: 8/2015 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Lemtrada
Lemtrada (alemtuzumab) Policy Number: 5.02.517 Last Review: 7/2018 Origination: 8/2015 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Lemtrada
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 6 April 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 6 April 2011 COPAXONE 20 mg/ml, solution for injection, pre-filled syringe B/28 (CIP code: 363 840-1) Applicant: SANOFI-AVENTIS
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 6 April 2011 COPAXONE 20 mg/ml, solution for injection, pre-filled syringe B/28 (CIP code: 363 840-1) Applicant: SANOFI-AVENTIS
S.E.A.R.C.H. SM Patient Workbook
 S.E.A.R.C.H. SM Patient Workbook How to S.E.A.R.C.H. SM for the Right MS Therapy For You! What is S.E.A.R.C.H. SM? The first treatment for relapsing-remitting multiple sclerosis (RRMS) was approved by
S.E.A.R.C.H. SM Patient Workbook How to S.E.A.R.C.H. SM for the Right MS Therapy For You! What is S.E.A.R.C.H. SM? The first treatment for relapsing-remitting multiple sclerosis (RRMS) was approved by
Update on New MS Therapeutics
 Update on New MS Therapeutics William Meador, MD Assistant Professor AAN August 2017 Meeting Disclosures Clinical Trial Involvement: SPRINT-MS Trial MediciNova, ibudilast LemCog Sanofi/Genzyme, alemtuzumab
Update on New MS Therapeutics William Meador, MD Assistant Professor AAN August 2017 Meeting Disclosures Clinical Trial Involvement: SPRINT-MS Trial MediciNova, ibudilast LemCog Sanofi/Genzyme, alemtuzumab
CADTH Canadian Drug Expert Committee Recommendation
 CADTH COMMON DRUG REVIEW CADTH Canadian Drug Expert Committee Recommendation (Final) GLATIRAMER ACETATE (GLATECT PENDOPHARM) Indication: Relapsing-Remitting Multiple Sclerosis RECOMMENDATION: The CADTH
CADTH COMMON DRUG REVIEW CADTH Canadian Drug Expert Committee Recommendation (Final) GLATIRAMER ACETATE (GLATECT PENDOPHARM) Indication: Relapsing-Remitting Multiple Sclerosis RECOMMENDATION: The CADTH
Technology appraisal guidance Published: 28 September 2016 nice.org.uk/guidance/ta407
 Secukinumab for active ankylosing spondylitis after treatment with non- steroidal anti-inflammatory drugs or TNF-alpha inhibitors Technology appraisal guidance Published: 28 September 16 nice.org.uk/guidance/ta407
Secukinumab for active ankylosing spondylitis after treatment with non- steroidal anti-inflammatory drugs or TNF-alpha inhibitors Technology appraisal guidance Published: 28 September 16 nice.org.uk/guidance/ta407
Supplementary Appendix A: Cost-effectiveness Model: Additional Input Parameter Values
 Supplementary Appendix A: Cost-effectiveness Model: Additional Input Parameter Values Appendix A: Cost-effectiveness Model: Additional Input Parameter Values Detailed Input Tables Table A.1: Annual Probability
Supplementary Appendix A: Cost-effectiveness Model: Additional Input Parameter Values Appendix A: Cost-effectiveness Model: Additional Input Parameter Values Detailed Input Tables Table A.1: Annual Probability
Boceprevir for the treatment of genotype 1 chronic hepatitis C
 Boceprevir for the treatment of genotype 1 chronic Issued: April 2012 guidance.nice.org.uk/ta NHS Evidence has accredited the process used by the Centre for Health Technology Evaluation at NICE to produce
Boceprevir for the treatment of genotype 1 chronic Issued: April 2012 guidance.nice.org.uk/ta NHS Evidence has accredited the process used by the Centre for Health Technology Evaluation at NICE to produce
Clinical Policy: Teriflunomide (Aubagio) Reference Number: CP.PHAR.262 Effective Date: Last Review Date: 05.18
 Reference Number: CP.PHAR.262 Effective Date: Last Review Date: 05.18") Clinical Policy: (Aubagio) Reference Number: CP.PHAR.262 Effective Date: 08.01.16 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Aubagio) Reference Number: CP.PHAR.262 Effective Date: 08.01.16 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Approved by: Pharmacy and Therapeutics Quality Management Subcommittee Effective Date: Department of Origin: Pharmacy. Date approved: 06/21/17
 Integrated Healthcare Services and Criteria Document: Reference #: PC/B016 Page: 1 of 4 PRODUCT APPLICATION: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA
Integrated Healthcare Services and Criteria Document: Reference #: PC/B016 Page: 1 of 4 PRODUCT APPLICATION: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Aubagio) Reference Number: CP.PHAR.262 Effective Date: 07.01.18 Last Review Date: 05.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Aubagio) Reference Number: CP.PHAR.262 Effective Date: 07.01.18 Last Review Date: 05.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end of this policy
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Ocrevus) Reference Number: CP.PHAR.335 Effective Date: 07.01.18 Last Review Date: 05.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Ocrevus) Reference Number: CP.PHAR.335 Effective Date: 07.01.18 Last Review Date: 05.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end of this policy
Clinical Policy: Ocrelizumab (Ocrevus) Reference Number: CP.PHAR.335 Effective Date: Last Review Date: 05.18
 Reference Number: CP.PHAR.335 Effective Date: Last Review Date: 05.18") Clinical Policy: (Ocrevus) Reference Number: CP.PHAR.335 Effective Date: 04.01.17 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Ocrevus) Reference Number: CP.PHAR.335 Effective Date: 04.01.17 Last Review Date: 05.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Tysabri) Reference Number: CP.CPA.206 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder at the end
Clinical Policy: (Tysabri) Reference Number: CP.CPA.206 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder at the end
Long term treatment of multiple sclerosis with interferon-beta may be cost effective Kendrick M, Johnson K I
 Long term treatment of multiple sclerosis with interferon-beta may be cost effective Kendrick M, Johnson K I Record Status This is a critical abstract of an economic evaluation that meets the criteria
Long term treatment of multiple sclerosis with interferon-beta may be cost effective Kendrick M, Johnson K I Record Status This is a critical abstract of an economic evaluation that meets the criteria
Beta interferon and glatiramer acetate for treating multiple sclerosis (review of TA32) [ID809]
![Beta interferon and glatiramer acetate for treating multiple sclerosis (review of TA32) [ID809]](/thumbs/80/81788237.jpg "Beta interferon and glatiramer acetate for treating multiple sclerosis (review of TA32) [ID809]") Please read the checklist for submitting comments at the end of this form. We cannot accept forms that are not filled in correctly. The Appraisal Committee is interested in receiving comments on the following:
Please read the checklist for submitting comments at the end of this form. We cannot accept forms that are not filled in correctly. The Appraisal Committee is interested in receiving comments on the following:
Including Real World Evidence (RWE) in network meta-analysis
 in network meta-analysis") Including Real World Evidence (RWE) in network meta-analysis David Jenkins, Reynaldo Martina, Sylwia Bujkiewicz, Pascale Dequen & Keith Abrams Department of Health Sciences, Background GetReal is a three-year
Including Real World Evidence (RWE) in network meta-analysis David Jenkins, Reynaldo Martina, Sylwia Bujkiewicz, Pascale Dequen & Keith Abrams Department of Health Sciences, Background GetReal is a three-year
Biogen Idec Neurology Pipeline. Alfred Sandrock, MD, PhD SVP, Neurology Research & Development
 Biogen Idec Neurology Pipeline Alfred Sandrock, MD, PhD SVP, Neurology Research & Development March 25, 2009 Robust Neurology Pipeline Neurology Multiple Sclerosis Discovery Pre-Clinical Phase 1 Phase
Biogen Idec Neurology Pipeline Alfred Sandrock, MD, PhD SVP, Neurology Research & Development March 25, 2009 Robust Neurology Pipeline Neurology Multiple Sclerosis Discovery Pre-Clinical Phase 1 Phase
Opexa Therapeutics, Inc.
 Opexa Therapeutics, Inc. November 2011 Neil Warma President & CEO Forward-Looking Statements This presentation contains forward-looking statements which are made pursuant to the safe harbor provisions
Opexa Therapeutics, Inc. November 2011 Neil Warma President & CEO Forward-Looking Statements This presentation contains forward-looking statements which are made pursuant to the safe harbor provisions
Tysedmus, a Registry of Multiple Sclerosis patients exposed to Natalizumab
 PHARMACOVIGILANCE AND REGISTRY PROGRAMMES Tysedmus, a Registry of Multiple Sclerosis patients exposed to Natalizumab Eric Van Ganse Pharmacoepidemiology, CHU-Lyon France OUTLINE I. GOOD REGISTRY PRACTICE
PHARMACOVIGILANCE AND REGISTRY PROGRAMMES Tysedmus, a Registry of Multiple Sclerosis patients exposed to Natalizumab Eric Van Ganse Pharmacoepidemiology, CHU-Lyon France OUTLINE I. GOOD REGISTRY PRACTICE
Modelling the cost effectiveness of interferon beta and glatiramer acetate in the management of multiple sclerosis
 Modelling the cost effectiveness of interferon beta and glatiramer acetate in the management of multiple sclerosis Jim Chilcott, Chris McCabe, Paul Tappenden, Anthony O Hagan, Nicola J Cooper, Keith Abrams,
Modelling the cost effectiveness of interferon beta and glatiramer acetate in the management of multiple sclerosis Jim Chilcott, Chris McCabe, Paul Tappenden, Anthony O Hagan, Nicola J Cooper, Keith Abrams,
Natalizumab (Tysabri) Humanized, MAb Against α 4 subunit of α 4 β 1 Integrin. Multiple Sclerosis Treatment Update
 Humanized, MAb Against α 4 subunit of α 4 β 1 Integrin. Multiple Sclerosis Treatment Update") Natalizumab (Tysabri) Humanized, MAb Against α 4 subunit of α 4 β 1 Integrin Complementarity-Determining Regions (CDRs) Multiple Sclerosis Treatment Update CDR grafted from murine Ab Human IgG 4 framework
Natalizumab (Tysabri) Humanized, MAb Against α 4 subunit of α 4 β 1 Integrin Complementarity-Determining Regions (CDRs) Multiple Sclerosis Treatment Update CDR grafted from murine Ab Human IgG 4 framework
Clinical Utility of Glatiramer Acetate in the Management of Relapse Frequency in Multiple Sclerosis
 Journal of Central Nervous System Disease Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Clinical Utility of Glatiramer Acetate in the Management
Journal of Central Nervous System Disease Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Clinical Utility of Glatiramer Acetate in the Management
Scottish Medicines Consortium
 Scottish Medicines Consortium interferon alfa 2b (Viraferon and Intron A* ) 18 million IU, solution for injection, multidose pen in combination with ribavirin (Rebetol ) capsules 200 mg No. (258/06) Schering
Scottish Medicines Consortium interferon alfa 2b (Viraferon and Intron A* ) 18 million IU, solution for injection, multidose pen in combination with ribavirin (Rebetol ) capsules 200 mg No. (258/06) Schering
2018 ECTRIMS Data Review Call. October 2018
 2018 ECTRIMS Data Review Call October 2018 TG Therapeutics Michael S. Weiss, CEO Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private
2018 ECTRIMS Data Review Call October 2018 TG Therapeutics Michael S. Weiss, CEO Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only.
 This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. Multiple Sclerosis Agents Ampyra Aubagio Avonex Betaseron Copaxone Extavia Gilenya Glatopa Plegridy Rebif Tysabri
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. Multiple Sclerosis Agents Ampyra Aubagio Avonex Betaseron Copaxone Extavia Gilenya Glatopa Plegridy Rebif Tysabri
SESSION VI THE CHALLENGE OF NEW TREATMENTS THE PHARMA INDUSTRY
 SESSION VI THE CHALLENGE OF NEW TREATMENTS THE PHARMA INDUSTRY Bruno C. Musch, MD PhD Baveno, Italy November 30th, 2013 DISCLOSURE OF INTEREST Dr.Musch is currently Medical Director in GENENTECH/Roche,
SESSION VI THE CHALLENGE OF NEW TREATMENTS THE PHARMA INDUSTRY Bruno C. Musch, MD PhD Baveno, Italy November 30th, 2013 DISCLOSURE OF INTEREST Dr.Musch is currently Medical Director in GENENTECH/Roche,
Prior Authorization Form
 5/2/2017 Prior Authorization Form INTOTAL HEALTH PLAN (SPC) Multiple Sclerosis MMT SGM This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
5/2/2017 Prior Authorization Form INTOTAL HEALTH PLAN (SPC) Multiple Sclerosis MMT SGM This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Cladribine. Spirella Building, Letchworth, SG6 4ET reg charity no
 Cladribine Spirella Building, Letchworth, SG6 4ET 01462 476700 www.mstrust.org.uk reg charity no. 1088353 Cladribine Date of issue: February 2009 Contents Section Page 1. Introduction 1 2. How cladribine
Cladribine Spirella Building, Letchworth, SG6 4ET 01462 476700 www.mstrust.org.uk reg charity no. 1088353 Cladribine Date of issue: February 2009 Contents Section Page 1. Introduction 1 2. How cladribine
Economic evaluation of Telaprevir (Incivo ) as add-on therapy to pegylated interferon and ribavirin for the treatment of patients infected with
 as add-on therapy to pegylated interferon and ribavirin for the treatment of patients infected with") Economic evaluation of Telaprevir (Incivo ) as add-on therapy to pegylated interferon and ribavirin for the treatment of patients infected with Hepatitis C Genotype 1. January 2012 Telaprevir Summary 1.
Economic evaluation of Telaprevir (Incivo ) as add-on therapy to pegylated interferon and ribavirin for the treatment of patients infected with Hepatitis C Genotype 1. January 2012 Telaprevir Summary 1.
Approval of a drug under this criteria document does not ensure full coverage of the drug.
 Criteria Document: Reference #: PC/B016 Page: 1 of 4 and Therapeutics Quality PRODUCT APPLICATIO: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne
Criteria Document: Reference #: PC/B016 Page: 1 of 4 and Therapeutics Quality PRODUCT APPLICATIO: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne
IR Thematic Call on Multiple Sclerosis
 Teresa, Multiple Sclerosis, United States IR Thematic Call on Multiple Sclerosis October 3 rd, 2013 Forward Looking Statements This presentation contains forward-looking statements as defined in the Private
Teresa, Multiple Sclerosis, United States IR Thematic Call on Multiple Sclerosis October 3 rd, 2013 Forward Looking Statements This presentation contains forward-looking statements as defined in the Private
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Multiple Sclerosis Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Multiple Sclerosis Agents Tysabri (natalizumab) and Lemtrada (alemtuzumab),
Multiple Sclerosis Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Multiple Sclerosis Agents Tysabri (natalizumab) and Lemtrada (alemtuzumab),
Multiple Sclerosis Agents Drug Class Prior Authorization Protocol
 Multiple Sclerosis Agents Drug Class Prior Authorization Protocol Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 This policy has been developed through review
Multiple Sclerosis Agents Drug Class Prior Authorization Protocol Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 This policy has been developed through review
CDEC FINAL RECOMMENDATION
 CDEC FINAL RECOMMENDATION APIXABAN (Eliquis Bristol-Myers Squibb Canada and Pfizer Canada) Indication: Venous Thromboembolic Events Recommendation: The Canadian Drug Expert Committee (CDEC) recommends
CDEC FINAL RECOMMENDATION APIXABAN (Eliquis Bristol-Myers Squibb Canada and Pfizer Canada) Indication: Venous Thromboembolic Events Recommendation: The Canadian Drug Expert Committee (CDEC) recommends
Disclosures and Acknowledgments
 214 Cooperative Meeting of the Consortium of Multiple Sclerosis Centers and Americas Committee for Treatment and Research in Multiple Sclerosis Dallas, Texas DX1 Disability Progression in Multiple Sclerosis
214 Cooperative Meeting of the Consortium of Multiple Sclerosis Centers and Americas Committee for Treatment and Research in Multiple Sclerosis Dallas, Texas DX1 Disability Progression in Multiple Sclerosis
Francesca Rinaldi, Paola Perini, Matteo Atzori, Alice Favaretto, Dario Seppi, and Paolo Gallo. 1. Introduction. 2. Materials and Methods
 Multiple Sclerosis International Volume 2015, Article ID 369348, 5 pages http://dx.doi.org/10.1155/2015/369348 Clinical Study Disease-Modifying Drugs Reduce Cortical Lesion Accumulation and Atrophy Progression
Multiple Sclerosis International Volume 2015, Article ID 369348, 5 pages http://dx.doi.org/10.1155/2015/369348 Clinical Study Disease-Modifying Drugs Reduce Cortical Lesion Accumulation and Atrophy Progression
Antibody therapy of multiple sclerosis Prof. Alastair Compston Dr. Alasdair Coles
 Antibody therapy of multiple sclerosis & Department of Clinical Neurosciences, School of Clinical Medicine, University of Cambridge, U.K. 1 The story of multiple sclerosis: 1838-1993 2 The symptoms of
Antibody therapy of multiple sclerosis & Department of Clinical Neurosciences, School of Clinical Medicine, University of Cambridge, U.K. 1 The story of multiple sclerosis: 1838-1993 2 The symptoms of
Outline. References. Marshall,1
 Outline Multiple Sclerosis: More Than Your ABC s Janene L. Marshall, PharmD, BCPS Clinical Associate Professor Internal Medicine Clinical Pharmacist Chicago State University College of Pharmacy J-marshall@csu.edu
Outline Multiple Sclerosis: More Than Your ABC s Janene L. Marshall, PharmD, BCPS Clinical Associate Professor Internal Medicine Clinical Pharmacist Chicago State University College of Pharmacy J-marshall@csu.edu
Dimethyl Fumarate and Peginterferon β-1a: New Insights Into the Pivotal Trials
 Dimethyl Fumarate and Peginterferon β-1a: New Insights Into the Pivotal Trials Pavan Bhargava, MD Johns Hopkins University School of Medicine, Baltimore, Maryland Abstract Treatment options for multiple
Dimethyl Fumarate and Peginterferon β-1a: New Insights Into the Pivotal Trials Pavan Bhargava, MD Johns Hopkins University School of Medicine, Baltimore, Maryland Abstract Treatment options for multiple
LEMTRADA (ALEMTUZUMAB)
") LEMTRADA (ALEMTUZUMAB) UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2017D0023O Effective Date: June 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
LEMTRADA (ALEMTUZUMAB) UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2017D0023O Effective Date: June 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Appraisal of Beta Interferon/ Glatiramer for Multiple Sclerosis Final Appraisal Determination
 Appraisal of Beta Interferon/ Glatiramer for Multiple Sclerosis Final Appraisal Determination Please note this document has been issued to consultees for the appeal period. It does not constitute guidance
Appraisal of Beta Interferon/ Glatiramer for Multiple Sclerosis Final Appraisal Determination Please note this document has been issued to consultees for the appeal period. It does not constitute guidance
Technology appraisal guidance Published: 19 July 2017 nice.org.uk/guidance/ta457
 Carfilzomib for previously treated multiple myeloma Technology appraisal guidance Published: 19 July 2017 nice.org.uk/guidance/ta457 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Carfilzomib for previously treated multiple myeloma Technology appraisal guidance Published: 19 July 2017 nice.org.uk/guidance/ta457 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
LEMTRADA (ALEMTUZUMAB)
") LEMTRADA (ALEMTUZUMAB) UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0023P Effective Date: April 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
LEMTRADA (ALEMTUZUMAB) UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0023P Effective Date: April 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Technology appraisal guidance Published: 23 January 2002 nice.org.uk/guidance/ta32
 Beta interferon and glatiramer amer acetate for the treatment of multiple sclerosis Technology appraisal guidance Published: 23 January 2002 nice.org.uk/guidance/ta32 NICE 2017. All rights reserved. Subject
Beta interferon and glatiramer amer acetate for the treatment of multiple sclerosis Technology appraisal guidance Published: 23 January 2002 nice.org.uk/guidance/ta32 NICE 2017. All rights reserved. Subject
Multiple Sclerosis: KOL Insight 2016
 Multiple Sclerosis: KOL Insight 2016 Multiple Sclerosis: KOL Insight 2016 BioPortfolio has been marketing business and market research reports from selected publishers for over fifteen years. BioPortfolio
Multiple Sclerosis: KOL Insight 2016 Multiple Sclerosis: KOL Insight 2016 BioPortfolio has been marketing business and market research reports from selected publishers for over fifteen years. BioPortfolio
The MS Disease- Modifying Medications. General information
 The MS Disease- Modifying Medications General information Current as of April 2013. This online brochure is updated with breaking news as required. If you have a printed a copy of this publication, please
The MS Disease- Modifying Medications General information Current as of April 2013. This online brochure is updated with breaking news as required. If you have a printed a copy of this publication, please
RESEARCH/CLINICAL UPDATE
 National Multiple Sclerosis Society 733 Third Avenue New York, New York 10017-3288 Tel +1 212.986.3240 Fax +1 212.986.7981 E-mail nat@nmss.org nationalmssociety.org October 30, 2007 RESEARCH/CLINICAL UPDATE
National Multiple Sclerosis Society 733 Third Avenue New York, New York 10017-3288 Tel +1 212.986.3240 Fax +1 212.986.7981 E-mail nat@nmss.org nationalmssociety.org October 30, 2007 RESEARCH/CLINICAL UPDATE
The Latest Therapies for MS: Weighing Respective Benefits and Risks
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/frontlines-multiple-sclerosis/the-latest-therapies-for-ms-weighingrespective-benefits-and-risks/9639/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/frontlines-multiple-sclerosis/the-latest-therapies-for-ms-weighingrespective-benefits-and-risks/9639/
Multiple sclerosis (MS) is a chronic, unpredictable
 is a chronic, unpredictable") Prescription Utilization by Multiple Sclerosis Patients in the United States Drug Trends Anna A. Theodorou, RPh, MBA; Kelly M. Johnson, MBA; Stacey Ruf, PhD; and John A. Szychowski, AAS, BS Multiple sclerosis
Prescription Utilization by Multiple Sclerosis Patients in the United States Drug Trends Anna A. Theodorou, RPh, MBA; Kelly M. Johnson, MBA; Stacey Ruf, PhD; and John A. Szychowski, AAS, BS Multiple sclerosis
Scottish Medicines Consortium
 Scottish Medicines Consortium fondaparinux sodium, 2.5mg/0.5ml solution for injection, pre-filled syringe (Arixtra ) No. (420/07) GlaxoSmithKline 09 November 2007 The Scottish Medicines Consortium has
Scottish Medicines Consortium fondaparinux sodium, 2.5mg/0.5ml solution for injection, pre-filled syringe (Arixtra ) No. (420/07) GlaxoSmithKline 09 November 2007 The Scottish Medicines Consortium has
Disease modifying therapies in multiple sclerosis
 Special Article Disease modifying therapies in multiple sclerosis Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the MS Council for Clinical
Special Article Disease modifying therapies in multiple sclerosis Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the MS Council for Clinical
Extending Our Leadership Position in Multiple Sclerosis. December 12, 2018
 Extending Our Leadership Position in Multiple Sclerosis December 12, 2018 1 Forward-Looking Statements This presentation contains forward-looking statements, including statements relating to: our strategy
Extending Our Leadership Position in Multiple Sclerosis December 12, 2018 1 Forward-Looking Statements This presentation contains forward-looking statements, including statements relating to: our strategy
Multiple Sclerosis International Federation December 2018
 MSIF WHO EML APPLICATION Multiple Sclerosis Disease-Modifying Therapies 1. Summary statement of the proposal for inclusion In 2015, an application for widening the indication of azathioprine to cover multiple
MSIF WHO EML APPLICATION Multiple Sclerosis Disease-Modifying Therapies 1. Summary statement of the proposal for inclusion In 2015, an application for widening the indication of azathioprine to cover multiple
Helen C. Pervanas, Pharm.D. Associate Professor of Pharmacy Practice MCPHS Worcester/Manchester
 Helen C. Pervanas, Pharm.D. Associate Professor of Pharmacy Practice MCPHS Worcester/Manchester helen.pervanas@mcphs.edu Objectives Describe the pathophysiology, diagnosis and prognosis of MS Discuss disease
Helen C. Pervanas, Pharm.D. Associate Professor of Pharmacy Practice MCPHS Worcester/Manchester helen.pervanas@mcphs.edu Objectives Describe the pathophysiology, diagnosis and prognosis of MS Discuss disease
Pipeline Drug Evidence Review: Ocrevus (ocrelizumab) vs. Tysabri, Lemtrada, Rebif and Tecfidera June 8, 2016
 vs. Tysabri, Lemtrada, Rebif and Tecfidera June 8, 2016") For more information contact us Pipeline Drug Evidence Review: Ocrevus (ocrelizumab) vs. Tysabri, Lemtrada, Rebif and Tecfidera June 8, 2016 Copyright. 2016 Advera Health Analytics, Inc. All rights reserved.
For more information contact us Pipeline Drug Evidence Review: Ocrevus (ocrelizumab) vs. Tysabri, Lemtrada, Rebif and Tecfidera June 8, 2016 Copyright. 2016 Advera Health Analytics, Inc. All rights reserved.
Economic evaluation of Avonex (interferon beta-1a) in patients following a single demyelinating event
 in patients following a single demyelinating event") 2005; 11: 542 /551 www.multiplesclerosisjournal.com Economic evaluation of Avonex (interferon beta-1a) in patients following a single demyelinating event Michael Iskedjian*,1, John H Walker 1,2, Trevor
2005; 11: 542 /551 www.multiplesclerosisjournal.com Economic evaluation of Avonex (interferon beta-1a) in patients following a single demyelinating event Michael Iskedjian*,1, John H Walker 1,2, Trevor
Evidence-Based Medicine What it Is. Critical Analysis of Clinical Trials Assessing Therapeutic Value
 Critical Analysis of Clinical Trials Assessing Therapeutic Value Douglas S. Goodin, M.D. Professor of Neurology, UCSF Any astronomer can predict just where every star will be at half past eleven tonight.
Critical Analysis of Clinical Trials Assessing Therapeutic Value Douglas S. Goodin, M.D. Professor of Neurology, UCSF Any astronomer can predict just where every star will be at half past eleven tonight.
MAY 2018 RESEARCH U P D A T E
 MAY 2018 MS RESEARCH U P D A T E MS RESEARCH U P D A T E Written and compiled by Tom Garry with Stephen Krieger, MD and Michelle Fabian, MD Reviewed by Jack Burks, MD Edited by Susan Courtney The 2018
MAY 2018 MS RESEARCH U P D A T E MS RESEARCH U P D A T E Written and compiled by Tom Garry with Stephen Krieger, MD and Michelle Fabian, MD Reviewed by Jack Burks, MD Edited by Susan Courtney The 2018
Clinical Policy: Multiple Sclerosis Reference Number: CP.CPA.206 Effective Date: Last Review Date: Line of Business: Commercial
 Clinical Policy: Reference Number: CP.CPA.206 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.206 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
NICE methods of technology appraisal
 NICE methods of technology appraisal Zoe Garrett Senior Technical Adviser, Centre for Health Technology Evaluation National Institute for Health and Care Excellence (NICE) Contents Function of NICE Work
NICE methods of technology appraisal Zoe Garrett Senior Technical Adviser, Centre for Health Technology Evaluation National Institute for Health and Care Excellence (NICE) Contents Function of NICE Work
Form 2043 R3.0: Multiple Sclerosis Pre-HSCT data
 Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: EBMT Center Identification Code (CIC): Today's Date: - - Date of HSCT for which this form is being completed: -
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: EBMT Center Identification Code (CIC): Today's Date: - - Date of HSCT for which this form is being completed: -
ISPOR 18th Annual European Congress Tuesday 10 November,13:45-14:45
 ISPOR 18th Annual European Congress Tuesday 10 November,13:45-14:45 Introduction Alastair Kent, OBE, Genetic Alliance UK, London, UK Recent HTA decisions Jacco Keja, PhD, IMS Health, Rotterdam, The Netherlands
ISPOR 18th Annual European Congress Tuesday 10 November,13:45-14:45 Introduction Alastair Kent, OBE, Genetic Alliance UK, London, UK Recent HTA decisions Jacco Keja, PhD, IMS Health, Rotterdam, The Netherlands
GetReal - Project No
 GetReal - Project No. 115546 WP1: Deliverable 1.5 (Case Study Review: Multiple Sclerosis) Lead Organisations: NICE, Novartis IMI GetReal Deliverable 1.5: Case Study on MS Disease and Treatment Overview
GetReal - Project No. 115546 WP1: Deliverable 1.5 (Case Study Review: Multiple Sclerosis) Lead Organisations: NICE, Novartis IMI GetReal Deliverable 1.5: Case Study on MS Disease and Treatment Overview
FORMULARY MANAGEMENT ABSTRACT
 FORMULARY MANAGEMENT Pharmacy Benefit Forecast for a New Interferon Beta-1a for the Treatment of Multiple Sclerosis: Development of a First-Line Decision Tool for Pharmacy-Budget Planning Using Administrative
FORMULARY MANAGEMENT Pharmacy Benefit Forecast for a New Interferon Beta-1a for the Treatment of Multiple Sclerosis: Development of a First-Line Decision Tool for Pharmacy-Budget Planning Using Administrative
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Multiple Sclerosis Agents Page 1 of 17 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Multiple Sclerosis Agents Tysabri (natalizumab) and Lemtrada (alemtuzumab)
Multiple Sclerosis Agents Page 1 of 17 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Multiple Sclerosis Agents Tysabri (natalizumab) and Lemtrada (alemtuzumab)
CIBMTR Center Number: CIBMTR Recipient ID: RETIRED. EBMT Center Identification Code (CIC): Today s Date:
: Today s Date:") Multiple Sclerosis Pre-HSCT Data EBMT Center Identification Code (CIC): Today s Date: Sequence Number: Date Received: Registry Use Only Date of HSCT for which this form is being completed: & 20 20 HSCT
Multiple Sclerosis Pre-HSCT Data EBMT Center Identification Code (CIC): Today s Date: Sequence Number: Date Received: Registry Use Only Date of HSCT for which this form is being completed: & 20 20 HSCT
Cost-effectiveness of oral agents in relapsing-remitting multiple sclerosis compared to interferon-based therapy in Saudi Arabia
 Cost-effectiveness of oral agents in relapsing-remitting multiple sclerosis compared to interferon-based therapy in Saudi Arabia Mai F. Alsaqa aby, a Varun Vaidya, b Noura Khreis, a Thamer Al Khairallah,
Cost-effectiveness of oral agents in relapsing-remitting multiple sclerosis compared to interferon-based therapy in Saudi Arabia Mai F. Alsaqa aby, a Varun Vaidya, b Noura Khreis, a Thamer Al Khairallah,
Todd Williamson VP US Medical Affairs, Data Generation & Observational Studies Bayer U.S. LLC
 Bayer wanted to ask why Betaseron is being included as one of the comparative agents for secondary progressive MS. Within the US Betaseron is not indicated for secondary progressive MS with minimal clinical
Bayer wanted to ask why Betaseron is being included as one of the comparative agents for secondary progressive MS. Within the US Betaseron is not indicated for secondary progressive MS with minimal clinical
Guide to the processes of technology appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guide to the processes of technology appraisal January 2018 Acknowledgements NICE is very grateful to everyone who contributed to the development of this
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guide to the processes of technology appraisal January 2018 Acknowledgements NICE is very grateful to everyone who contributed to the development of this
Drug Name (select from list of drugs shown) Tysabri (natalizumab) Quantity Frequency Strength Route of Administration
 Tysabri (natalizumab) Quantity Frequency Strength Route of Administration") 04/30/2014 Prior Authorization Form MERCY CARE PLAN (MEDICAID) Tysabri (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
04/30/2014 Prior Authorization Form MERCY CARE PLAN (MEDICAID) Tysabri (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and
DIAGNOSTICS ASSESSMENT PROGRAMME
 Diagnostics Consultation Document s THEME: LEVEL OF EVIDENCE 1. Section Response 1. Provisional Recommendations (page 2) Biomedical, Inc., the manufacturer of the My5-FU assay, is disappointed in the draft
Diagnostics Consultation Document s THEME: LEVEL OF EVIDENCE 1. Section Response 1. Provisional Recommendations (page 2) Biomedical, Inc., the manufacturer of the My5-FU assay, is disappointed in the draft
Mycophenolate mofetil in combination with interferon beta-1a in the treatment of relapsing-remitting multiple sclerosis: a preliminary study
 Received: 20.6.2010 Accepted: 5.8.2010 Original Article Mycophenolate mofetil in combination with interferon beta-1a in the treatment of relapsing-remitting multiple sclerosis: a preliminary study Masoud
Received: 20.6.2010 Accepted: 5.8.2010 Original Article Mycophenolate mofetil in combination with interferon beta-1a in the treatment of relapsing-remitting multiple sclerosis: a preliminary study Masoud
Timing is Everything: The Importance of Early Intervention in Multiple Sclerosis
 Timing is Everything: The Importance of Early Intervention in Multiple Sclerosis Challenge Question: Pathophysiology Which of the following is a correct statement about the pathophysiology of MS and/or
Timing is Everything: The Importance of Early Intervention in Multiple Sclerosis Challenge Question: Pathophysiology Which of the following is a correct statement about the pathophysiology of MS and/or
Scottish Medicines Consortium
 Scottish Medicines Consortium Guidance to Manufacturers for Completion of New Product Assessment Form (NPAF) (Revised June 2007) Part A: General guidance for completion of the NPAF Part B: Guidance for
Scottish Medicines Consortium Guidance to Manufacturers for Completion of New Product Assessment Form (NPAF) (Revised June 2007) Part A: General guidance for completion of the NPAF Part B: Guidance for
The challenges of preparing evidence for decision modelling. Marta Soares Centre for Health Economics, University of York
 The challenges of preparing evidence for decision modelling Marta Soares Centre for Health Economics, University of York MRC biostats 10/02/2015 Overview Context Overview of decision modelling Overview
The challenges of preparing evidence for decision modelling Marta Soares Centre for Health Economics, University of York MRC biostats 10/02/2015 Overview Context Overview of decision modelling Overview
Antihemophilic Factor (Recombinant BDD) Fc Fusion Protein (Eloctate): Treatment Cost Comparison and Budget Impact Analysis
 Fc Fusion Protein (Eloctate): Treatment Cost Comparison and Budget Impact Analysis") CADTH TECHNOLOGY REVIEW Antihemophilic Factor (Recombinant BDD) Fc Fusion Protein (): Treatment Cost Comparison and Budget Impact Analysis Product Line: Technology Review Version: 1.0 Issue Number: 2 Publication
CADTH TECHNOLOGY REVIEW Antihemophilic Factor (Recombinant BDD) Fc Fusion Protein (): Treatment Cost Comparison and Budget Impact Analysis Product Line: Technology Review Version: 1.0 Issue Number: 2 Publication
ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis
 EAN GUIDELINES/CME ARTICLE ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis X. Montalban a, R. Gold b, A. J. Thompson c, S. Otero-Romero a,d, M. P. Amato e, D. Chandraratna
EAN GUIDELINES/CME ARTICLE ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis X. Montalban a, R. Gold b, A. J. Thompson c, S. Otero-Romero a,d, M. P. Amato e, D. Chandraratna