New Drugs in the Sky: Coatings & Drug Elution for Improving Stents and Vascular Prostheses Beat H. Walpoth, MD
|
|
|
- Claude Burns
- 5 years ago
- Views:
Transcription




1 New Drugs in the Sky: Coatings & Drug Elution for Improving Stents and Vascular Prostheses Beat H. Walpoth, MD Department of Cardiovascular Surgery, University Hospital of Geneva, Switzerland
2 Coatings & Drug Elution for Improving Stents and Indications Vascular Prostheses Systemic: anticoagulation / antiaggregation Local: coating / drug release Passive surface coating: titanium Active surface coating: CD34 Drug Elution: VEGF Degradable DE Polymers: paclitaxel Biologic solution: endothelial seeding


")

3 Clinical needs PROBLEM Clinical needs replacements of small-caliber blood vessels per year in the US Autologous vascular material : lowest failure rate availibility (previous surgery) suitability (vascular disease) Synthetic vascular material : biostable (e-ptfe, Dacron ) large diameter > 6 mm small diameters < 6 mm acute thrombogenicity aneurysms intimal hyperplasia endothelialization 1
4 PASSIVE COATINGS Gold Heparin Carbon Silicon carbide Titanium Phosphorylcholine Cikirikcioglu M, Sedelnikov N, Osorio-da Cruz S, Khabiri E, Antal AD, Tatar T, Tille JC, Hess OM, Kalangos A, Walpoth BH. Improved neo-endothelialisation of small synthetic grafts with titanium coating. Int J Art Organs 2006 Vol. 29(10):990-99


5 AIM The aim of this study was to assess the effect of titanium coating on eptfe grafts and to assess short term patency, endothelialisation and intimal proliferation of these grafts. NATIVE PTFE TITANIUM COATED PTFE
 test was used to check")
.")
 (10 000 IU IV;")
6 METHOD- Thrombogenicity test Femoro-femoral ex vivo arterio-venous shunt (AVS) test was used to check thrombogenicity, cellular deposition and coating stability on grafts (in five pigs). Grafts were perfused for 9 minutes after heparinization (flow and pressure were monitored) ( IU IV; >double ACT) Pressure monitoring Flow monitoring


7 RESULTS- Thrombogenicity test Titanium coated eptfe grafts had lower thrombogenicity and cell deposition scores % of native PTFE Total Thrombogenicity Cell Deposition Titanium * *p < 001 NATIVE PTFE TITANIUM COATED PTFE
. The 10 grafts were either uncoated (n=5), or titanium coated (n=5). Each pig served as its own control.")
8 METHOD- Pig carotid artery interposition Pig carotid artery interposition model was used to check for chronic patency, endothelialisation and intimal hyperplasia. Bilateral carotid graft interposition was performed in 5 pigs (eptfe, 4mm ID, 50mm long). The 10 grafts were either uncoated (n=5), or titanium coated (n=5). Each pig served as its own control. (Carotid eptfe graft interposition) PROXIMAL ANASTOMOSIS DISTAL ANASTOMOSIS
 angiography was performed to check patency")


9 METHOD- Pig carotid artery interposition At the end of the study (30 3 days) angiography was performed to check patency and quantitative stenosis scores. Then grafts were excised for histology and scanning electron microscopy. Computed morphometry was carried out to determine intimal hyperplasia and percentage of cellular graft coverage. Titanium coated eptfe
 for titanium coated than uncoated grafts.")
10 RESULTS- Pig carotid artery interposition At 1 month, patency rate was 80% for native and titanium coated grafts. Morphometry revealed a significantly higher cellular coverage (CD 31+ cells) for titanium coated than uncoated grafts. There was a trend towards increased intimal hyperplasia in titanium coated compared to uncoated grafts.



11 ENDOTHELIAL COVERAGE ASSESSMENT OF TITANIUM COATING Cd 31 picture cripta and cells HE, x200 HE, x400 CD 31 staining, x200
12 DRUG-ELUTING BIODEGRADABLE POLYMERS Fibrin VEGF: BH Walpoth, P Zammaretti, M Cikirikcioglu, E Khabiri, MK Djebaili, J-C Pache, J-C Tille, Y Aggoun, D Morel, A Kalangos, JA Hubbell, AH Zisch. Enhanced Intimal Thickening of Expanded Polytetrafluoroethylene grafts coated with Fibrin or Fibrin-releasing Vascular Endothelial Growth Factor in the Pig Carotid Artery Interposition Model. J Thorac Cardiovasc Surg 2007;133:




* coating for")

13 Aim: The purpose of our study was to promote cellular coverage of vascular grafts by using slow release vascular endothelial growth factor-a (VEGF- 121 )* coating for rapid neo-endothelialisation. *Zisch A. Circ Res 2004; 98:
 were")
, fibrin")
")


")
14 The 28 grafts (2 for each pig) were used as native (n=10), fibrin (n=9) or fibrin + VEGF 121 (n= 9) coated. NON-COATED PTFE FIBRIN + VEGF COATED PTFE Scanning electron microscopic (SEM) pictures of materials before interposition x 800










15 Biologic coating stability test Fibrin Oregon Green Staining Before perfusion After 30 min perfusion






16 One month patency rate in uncoated control grafts is 70 % compared to 77 % in the fibrin and fibrin+vegf coated grafts respectively. Non-coated eptfe Fibrin coated eptfe Fibrin + VEGF coated eptfe Variance analysis* Patency 7/10 7/9 7/9 NS



,")
 and")

17 The angiographic narrowing in the middle of the graft ranged between 25 % (uncoated), 19 % (fibrin coated) and 25 %(fibrin+ VEGF 121 coated) groups.






18 Quantitative angiography (QCA) showed a significant difference at the proximal anastomosis between the noncoated and the coated groups. Stenosis % Non-coated eptfe Fibrin coated eptfe Fibrin + VEGF coated eptfe Variance analysis* Prox.Anast ,034** Middle Graft NS Dist. Anast NS Dist.Nat.Art NS *: Kruskal Wallis variance analysis **: p<0.05 (Mann Whitney U test)(non coated vs fibrin and fibrin + VEGF
19 Morphometry revealed significantly higher intimal hyperplasia in the fibrin + VEGF coated grafts when compared to uncoated grafts(overall and anastomosis) Non-coat. eptfe Fibrin coat. eptfe Fibrin+VEGF coated eptfe Variance analysis* Intimal hyperplasia (µm2/µm) 167,4 170,5 210,2 148,4 267,2 174,1 0,031** Cellular graft coverage ( % ) 80,0 20,1 82,7 17,6 89,9 14,8 NS *: Kruskal Wallis variance analysis **: p=0.008 (Mann Whitney U test)(non-coated vs fibrin + VEGF)
 FIBRIN + VEGF")

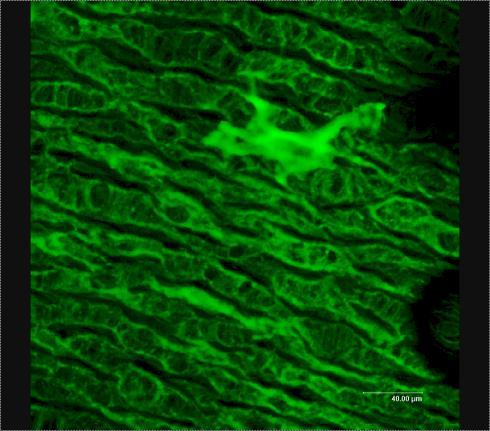
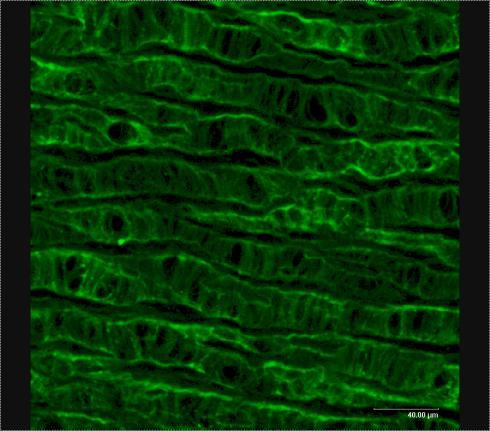
20 NON-COATED PTFE Neo-intimal graft coverage (mid-portion) FIBRIN + VEGF COATED PTFE Scanning electron microscopic pictures of grafts after 1 month

21 Neo-endothelium and intimal hyperplasia at 1 month
22 DRUG-ELUTING BIODEGRADABLE POLYMERS PCL-Paclitaxel: Innocenti F, Mandracchia D, Pektok E, Nottelet B, Tille J-C, de Valence S, Faggian G, Mazzucco A, Kalangos A, Gurny R, Moeller M, Walpoth BH. Paclitaxel-Eluting Biodegradable Synthetic Vascular Prostheses: A step towards reduction of neointima formation? Circulation. 2009;120[suppl 1]:S37 S45


23 GENERAL REQUIREMENTS for VTE Biofunctionality: Biocompatibility Extra Cellular Matrix Like Sterilization Ease of surgical handling Biodegradable polymers ELECTROSPINNING Biodegradability : Degradation of the graft AND simultaneous replacement by native tissues Non toxic byproducts


24 Electrospinning Polymer Solution Syringe Pump Ejection Needle High voltage
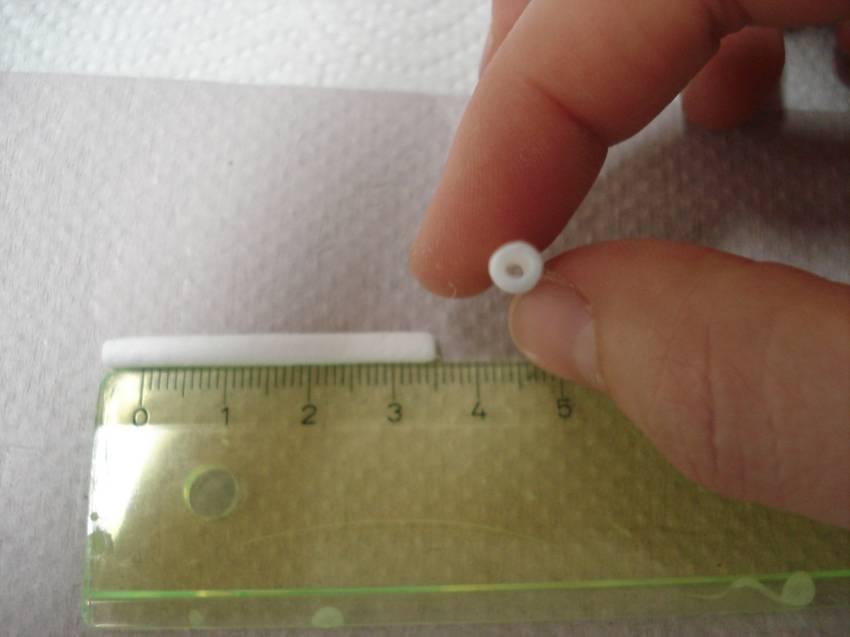



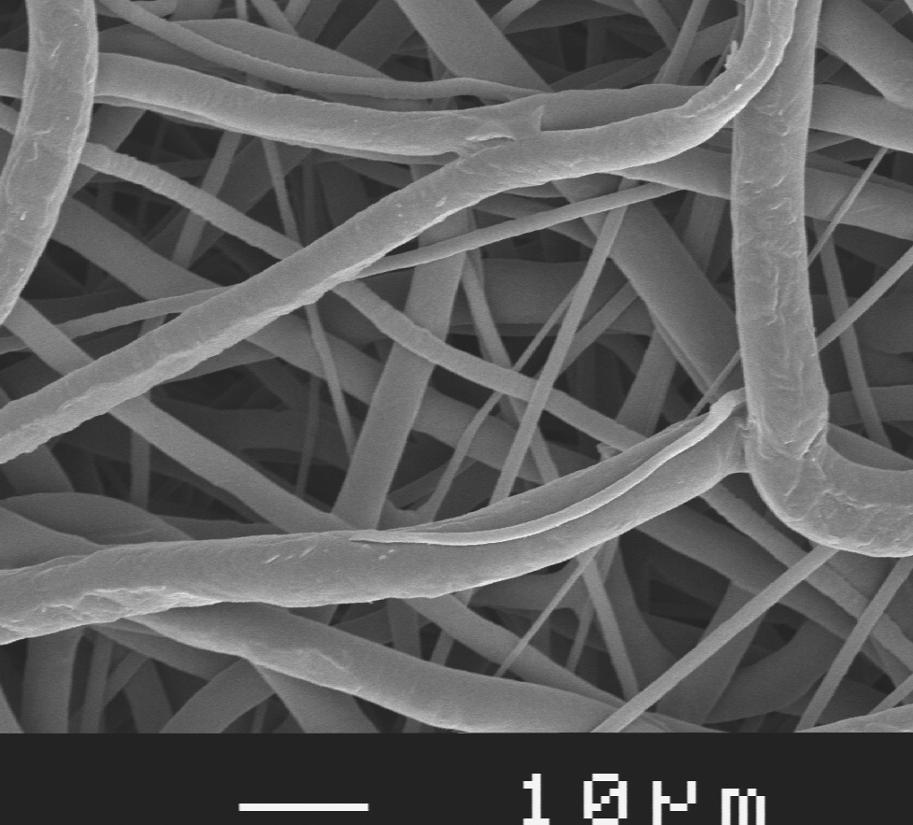

25 ELECTROSPINNING Nottelet B et al, J Biomed Mater Res 89A: , 2009 Small sized vascular graft (Ø 2mm) ECM-like structure Porosity c.a 80% Fibers Ø [50nm-5µm] Pores Ø [5μm -300μm] No in vitro cell-seeding needed




26 Quality and patency control after surgery with transit time flowmeter RAT ABDOMINAL AORTA PROSTHETIC REPLACEMENT 1mm diameter grafts were interposed in the infrarenal abdominal aorta under general anaesthesia. The anastomoses were performed with 10/0 interrupted nylon sutures with an operative microscope. Patency assessment was performed intra-operatively with transit time flow measurement in all animals. eptfe graft 1 mm PDS graft
 digital substraction")


27 ANGIOGRAPHIC PATENCY EVALUATION At conclusion of the study (1 year) digital substraction angiography was performed and grafts were harvested for morphologic as well as scanning electron microscopic examination. Rat 24 3 weeks after operation Rat 24 3 weeks after operation






28 IN VIVO PCL GRAFT RESULTS 6 Months PCL grafts vs eptfe grafts as Abdominal Aorta Substitutes in Rats A: PCL graft Very good surgical handling Fully patent at 24 weeks No aneurysmatic dilatation No stenosis DSA 24 weeks late B: eptfe graft Significant stenosis (70%-80%) in 1 in 3 cases A (Pektok E et al, Circulation. 2008;118: ) B
")
 IN VIVO PCL")


 Confluent")
")

29 Neointima area / length ( m m) Endothelial coverage (%) IN VIVO PCL GRAFT RESULTS 6 Months PCL grafts vs eptfe grafts (Pektok E et al, Circulation. 2008;118: ) Confluent endothelial layer PCL 24 weeks (x100) Angiogenesis IN VIVO PCL DEGRADATION Time of of implantation (weeks)



30 HYPOTHESIS Paclitaxel is cytostatic at low doses, blocking SMC proliferation* Paclitaxel Hyperplasia No hyperplasia Mechanical properties? Electrospinning device Drug release/activity? Innocente F et al, Circulation. 2009: 120;S37-S45
")

31 IN VITRO IN VITRO DRUG RELEASE PBS-Tween20 (37 C) Controlled drug release over 30 days Very low initial burst
32 IN VIVO NEO-INTIMA AREA 0,08 0,07 7a. Neo-intima area to total graft length ratio. PCL graft PCL-PTX graft [mm 2 /mm] 0,06 0,05 0,04 0,03 * p=0,049 # p=0,046 ##p=0,046 ^ p=0,037 * # * ## 0,02 ^ 0,01 0,00 # ## ^ Time [weeks]

33 COLLABORATIONS Faculty of Medicine Faculty of Science Local EPGL, Faculty of Science Department of Cardiology Department of Pathology Faculty of Dentistry, SEM Laboratory Experimental Anaesthesia Unit National EPFL ETHZ University of Bern International - University of Genova, Italy - University of Verona, Italy Harvard University, USA University of Virginia, USA


34 THANK YOU Don t dream your life - live your dream!