Advances in Stem Cell Transplant for Multiple Myeloma - The Shift to Outpatient Therapy. Gail Sulski, RN, MS, FNP, AOCNP
|
|
|
- Erika Hodges
- 5 years ago
- Views:
Transcription


1 Advances in Stem Cell Transplant for Multiple Myeloma - The Shift to Outpatient Therapy Gail Sulski, RN, MS, FNP, AOCNP
2 What s New in Myeloma? Shift to Outpatient Transplant New Drugs with higher remission rates Role of Maintenance Therapy Does Allogeneic transplant still play a role?
3 Stem Cell Transplant
4

5 Advantages Autologous Transplants -Does not require finding a donor -No risk of Graft Versus Host Disease (GVHD) -Decreased morbidity & mortality -Earlier engraftment* -Less costly -Age Disadvantages -Possible contamination with tumor cells -Lack of graft versus tumor responses
 bone marrow")
6 What Is It? Highly specialized procedure 2 major parts Destroy (malfunctioning) bone marrow w/chemo +/- TBI Replace bone marrow with functioning stem cells Stem cell rescue
7 Autologous Stem Cell Transplant High doses of chemotherapy Use stem cells to recover Cytopenic Phase (need for transfusions, antibiotics, pain control) Late complications rare One or two? When?
8 Pre-Transplant Workup Insurance approval* H & P* MUGA/ECHO* PFT S* Radiology as appropriate* (skeletal survey) HIV, Hepatitis, CMV* CBC, CMP, Lipid panel* ABO/HLA Dental evaluation* Psychological evaluation/sw* Colonoscopy >50 Bone marrow biopsy* PSA, mammogram, PAP/gyne exam PS* Caregiver?* Disease-dependent

9 Autologous Mobilization (Priming) <10% plasma cells in marrow Growth factors +/- chemotherapy causes large # of stem cells to be released from the bone marrow into the bloodstream Cyclophosphamide (1.5, 2, or 4 gm/m 2 ) Day 1 G-CSF 10 mcg/kg daily; start Day 6 Outpatient

10 Apheresis Collection of peripheral stem cells A portion of blood is separated & retained Remainder is returned to pt or donor Goal: collect enough for 2 transplants

11 Apheresis
12 Cryopreservation Process of storing the collected stem cells & maintaining viability while in storage -150 degrees celsius DMSO

13 Cryopreservation
14 Cryopreservation
")
15 Conditioning Regimens High-dose chemotherapy +/- total body irradiation (TBI) Eradicate the disease Suppress the immune system Open spaces in bone marrow to allow for engraftment Minus days (e.g., Melphalan Day -2 & Day -1)
16 Outpatient Transplants Better antibiotics, antinausea medications, mobilization techniques, nursing care Melphalan well tolerated as outpatient (dose reduced for >70 yrs old, comorbidities); cryotherapy Advances in mobilization lead to fewer collections and fewer side effects during reinfusion Day 0 Early days typically with minimal side effects Availability of 24/7 call

17 Reinfusion Stem cells are returned to the pt after myeloablative or submyeloablative therapy Day 0 Days after reinfusion are plus days (e.g., Day+1, +2, +3) Inpatient or outpatient
18 Outpatient Transplants Seen by NP in outpatient clinic Antiviral and antifungal Day +1 IVF s, antiemetics, antibiotics, Neupogen (G-CSF) Day +5 Transfusions as needed Follow-up visits based on blood counts, side effects experienced
19 Transplant: New & Improved Stem Cell Source Bone Marrow PBPC Type Inpatient Outpatient Median Age ANC Recovery 18 Days 11 Days Plt Recovery 22 Days 14 Days Length of Stay 3-4 weeks 6 days Mortality 2-5 % < 1%
 24 8 67% 7.")
20 Multiple Myeloma Outcomes All Myeloma Patients Myeloma < 70 Years of Age Myeloma >70 Years of Age N Admitted > 1 Day %TX Solely Outpatient LOS (Median Range) % 7.5 Days (4-24) % 5 Days (4-7) % 9 Days (8-24)

21
22 New Drugs Proteasome Inhibitors: Bortezomib, Carfilzomib (5 th new MM drug in 10 yrs!!) Immunomodulatory Agents: Lenalidomide, Thalidomide, Pomalidomide Monoclonal antibodies New combinations of drugs Different side effect profiles
23 Role of Maintenance New Drugs lead to better CR rates prior to BMT Transplant Improves on CR Maintenance now of proven benefit Which drug for maintenance?
24 Lenalidomide as Maintenance After ASCT McCarthy PL et al. N Engl J Med 2012;366:
25 In the Era of Novel Agents is There Still a Role for Transplantation? Response rates following induction with novel agents are higher than older approaches, even with high-risk disease Do we still need transplant with these improved responses? Early vs late? 1 vs 2? Studies ongoing IMWG recommends that auto SCT be offered at some point in the course of treatment for transplant-eligible patients 25
26 Event-free Survival According to Treatment Group Attal, M. et al. N Engl J Med 1996;335:91-97
27 Overall Survival According to Treatment Group Attal, M. et al. N Engl J Med 1996;335:91-97
28 What About Allo?

29 Allogeneic Transplants Advantages -No contamination with tumor cells -Graft-versus-tumor reaction Disadvantages -GVHD -Graft rejection -Substantial morbidity/mortality -Donor availability -Age

30 Allo: A Highly Specialized Procedure Preadmission Donor search or priming/collection Delivery or cryopreservation Conditioning Reinfusion Engraftment & Medical management Discharge Follow-up
 Toxicity due to")

")

31 Hospital Course Profound aplasia (neutropenia, thrombocytopenia, anemia) Toxicity due to conditioning regimen Nausea/vomiting Alopecia Skin rash Mucositis Analgesics Bacterial, fungal & viral prophylaxis/treatment sepsis, pneumonia Blood product support TPN Graft vs Host Disease (GVHD) prophylaxis/treatment Veno-Occlusive Disease (VOD) prophylaxis Psychosocial support Engraftment & resolution of toxicities
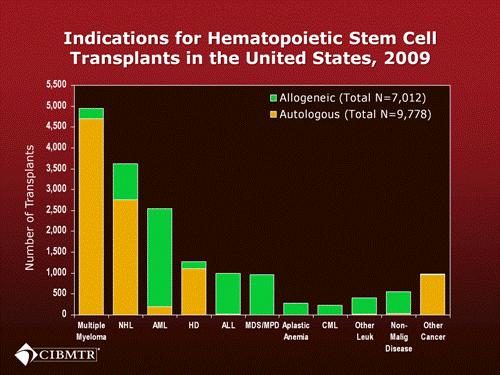
32 Probability of Survival, % Probability of survival after transplant for multiple myeloma, by donor type P < autologous transplant (N=22,254) HLA-matched sibling, Allo (N=878) Unrelated, Allo (N=143) Years Slide 49 SUM10_56.ppt
33 Conclusions Transplant still plays a key role in treatment of patients with myeloma (allo for select few) Transplant is safer and more tolerable than ever before Patients living longer with better QOL Newer therapies Maintenance therapy: which drug? how long?

34 Thank you!