BATTLING BUGS: INROADS IN INFECTIOUS DISEASES
|
|
|
- Roderick Garey Jennings
- 5 years ago
- Views:
Transcription
1 UW MEDICINE PATIENTS ARE FIRST BATTLING BUGS: INROADS IN INFECTIOUS DISEASES UW MINI-MEDICAL SCHOOL Brad T. Cookson M.D., Ph.D. February 11, 2014
2 FEVER: THE HOST RESPONDS Humanity has but three great enemies: fever, famine and war; of these by far the greatest, by far the most terrible, is fever. Sir William Osler,
3 HOUSTON, WE VE HAD A PROBLEM. 3

4 HOUSTON, WE VE HAD A PROBLEM. Four Leading Causes of Morbidity and Mortality: Heart Disease Stroke Cancer Infection 4
5 DIAGNOSIS: KEY TO EFFECTIVE TREATMENT Diagnosis. The determination of the nature of a disease. [G. a deciding] SYN: diacrisis. Diacrisis SYN: diagnosis [G. dia-, through, + krisis, a judgment] 5
6 DIAGNOSIS: KEY TO EFFECTIVE TREATMENT Listen to your patient, he is telling you the diagnosis. Sir William Osler ( ) 6
7 DIAGNOSIS: A SCIENTIFIC APPROACH Hypothesis testing: History Physical Exam (imaging) Laboratory Testing (Laboratory Medicine) 7
8 DEPARTMENT OF LABORATORY MEDICINE Chemistry Hematology Transfusion Medicine Immunology Microbiology Virology Medical Informatics Molecular Diagnosis Program (Molecular Microbiology Laboratory) 8
9 DEPARTMENT OF LABORATORY MEDICINE Chemistry Hematology Transfusion Medicine Immunology Microbiology Virology Medical Informatics Molecular Diagnosis Program (Molecular Microbiology Laboratory) Google: UW Medical Laboratory Science 9
10 IDENTIFY ETIOLOGICAL AGENTS Determine the nature of disease: Predict course and potential outcome(s) of infection Tailor therapy Exclude non-infectious cause(s) of symptoms 10
11 IDENTIFY ETIOLOGICAL AGENTS Determine the nature of disease: Predict course and potential outcome(s) of infection Tailor therapy Exclude non-infectious cause(s) of symptoms What you can t see, can kill you! 11
12 TRADITIONAL APPROACH If it grows, it can usually be identified 12
13 TRADITIONAL APPROACH If it grows, it can usually be identified Acquire patient specimen blood, urine, CSF Microscopic examination 13

14 TRADITIONAL APPROACH If it grows, it can usually be identified Acquire patient specimen blood, urine, CSF Microscopic examination Isolate Amplify 14

15 ISOLATE & AMPLIFY 15


16 ISOLATE & 10 9 AMPLIFICATION (Google: Scale of universe; Powers of Ten) 16
17 IDENTIFY ETIOLOGICAL AGENTS Phenotype (physical expression of genotype) Identification Antibiotic resistance Gene products (proteins, enzymes, complex structures) 17
18 IDENTIFY ETIOLOGICAL AGENTS Phenotype (physical expression of genotype) Identification Antibiotic resistance Gene products (proteins, enzymes, complex structures) Genotype (blueprint for phenotype) 18
19 TRADITIONAL APPROACH If it grows, it can usually be identified What if it grows very slowly? it does not grow in the lab? it has disguised usual characteristics? it has never been seen before? 19
20 TRADITIONAL APPROACH If it grows, it can usually be identified What if it grows very slowly? it does not grow in the lab? it has disguised usual characteristics? it has never been seen before? If it grows, it can usually be identified 20
21 IDENTIFY ETIOLOGICAL AGENTS Phenotype (physical expression of genotype) Identification Antibiotic resistance Gene products (proteins, enzymes, complex structures) Genotype (blueprint for phenotype) 21
22 GENOMIC APPROACH: ISOLATE & AMPLIFY Target: Species-identifying DNA sequences flanked by conserved primer binding sites 22
23 GENOMIC APPROACH: ISOLATE & AMPLIFY Target: Species-identifying DNA sequences flanked by conserved primer binding sites 23
24 CASE 1 79-yr-old male Soft-tissue excision Inflammatory tissue No microbial elements Cultures were negative 24
25 CASE 1 The differential diagnosis includes: infectious process (possible infection), inflammatory process such as rheumatoid nodule or a neoplastic process (epithelioid carcinoma can present with foci of necrosis, however the histopathological features do not favor same). PCR and DNA sequencing were performed on a PET specimen. 25

26 CASE 2 23-yr-old man with refractory seizures MRI: Vasogenic edema Gadolinium enhancing 26
27 CASE 2 Exhaustive serological testing was negative Cultures were negative Surgically excised lesion Mixed inflammatory cell infiltrate without presence of microbial elements PCR and DNA sequencing were performed on a fresh surgical specimen. 27

28 CASE 3 Young person with AML Lymph node biopsy Cultures negative PCR and DNA sequencing were performed. 28
29 GENOMIC APPROACH: ISOLATE & AMPLIFY Target: Species-identifying DNA sequences flanked by conserved primer binding sites 29
30 GENOMIC APPROACH: ISOLATE & AMPLIFY Target: Species-identifying DNA sequences flanked by conserved primer binding sites What if infection occurs at a site with normal microbiota? more than one pathogen is present? 30
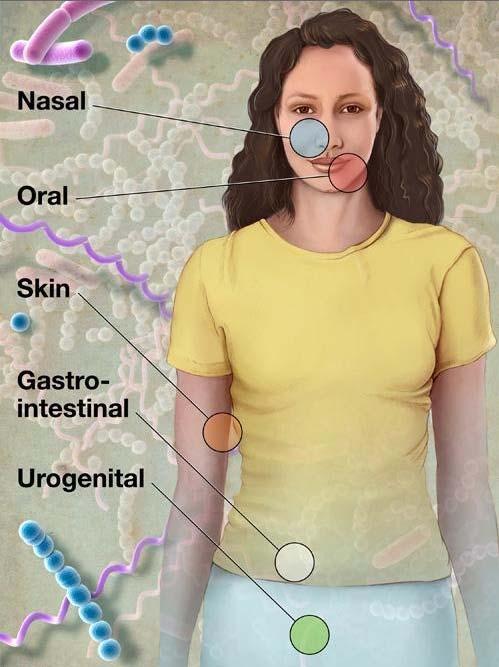
31 NORMAL MICROBIOTA 31
:193.")
32 POLYMICROBIAL INFECTION Clin. Microbiol. Rev. 2012, 25(1):
33 NEXT GENERATION SEQUENCING Sequencing the genome at 10 9 base pairs per second Dr. Toby Russell, assisted by Dr. Beverly Crusher, Genitronic replication of Worf s new spinal column, Episode #115, Star Trek, The Next Generation 33

34 NGS: ISOLATE & AMPLIFY Capture single DNA molecules Cluster formation: amplify ~1,000 copies Parallel DNA sequencing of clusters Read millions of clusters per flow cell! 34

35 BACTERIAL VAGINOSIS 35

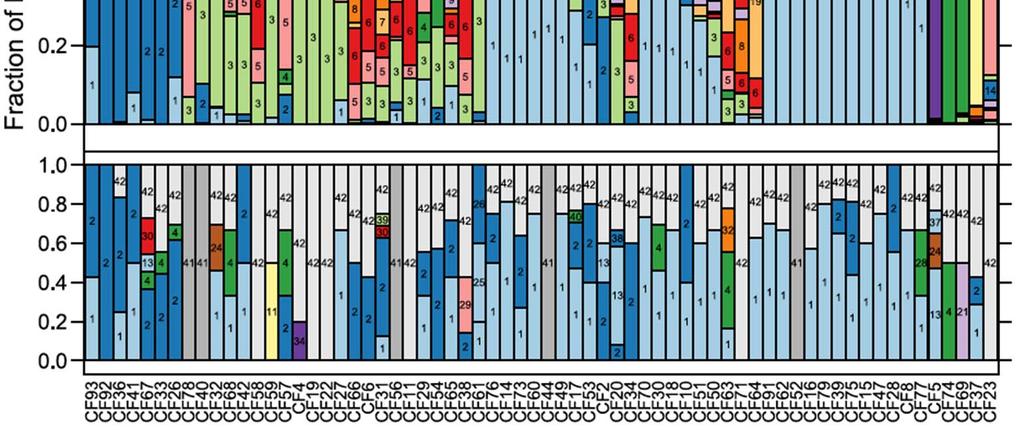
36 CYSTIC FIBROSIS 36
37 CASE 35-yr-old male with meningitis Found to have brain abscess CSF cultures were negative Traditional PCR + DNA sequencing revealed polymicrobial infection 37
38 CASE 35-yr-old male with meningitis Found to have brain abscess CSF cultures were negative Traditional PCR + DNA sequencing revealed polymicrobial infection Next Generation Sequencing was performed Antibiotic regimen was optimized 38
39 MOLECULAR MICROBIOLOGY LABORATORY Mission Support delivery of the best possible patient care by providing excellence in the laboratory science of diagnosing infectious diseases. 39

40 Google: UW Molecular Microbiology 40