Diagnosi delle infezioni opportunistiche nella nuova era della microbiologia
|
|
|
- Chester Stevens
- 5 years ago
- Views:
Transcription


1 Diagnosi delle infezioni opportunistiche nella nuova era della microbiologia Maurizio Sanguinetti Institute of Microbiology Fondazione Policlinico Universitario «A. Gemelli» - IRCCS
2 Rapid diagnostic methods in clinical microbiology: a game changer In most clinical labs, microbiology is performed by the way Louis Pasteur did it in Specimens are cultured on seaweed and incubated and, hours later, whatever has grown is identified. The introduction of molecular methods for microbial detection represents a quantum leap into the 21st century, having bypassed the 20th century almost completely. Perhaps the best example of use of this technology is the rapid detection of Mycobacterium tuberculosis, which permits conclusions about diagnosis and treatment of tuberculosis (the second most common infectious disease cause of death on earth) in less than 2 hours compared with standard techniques that generally require 4 6 weeks.
3 Rapid diagnostic methods in clinical microbiology: a game changer The rapid detection technology in Clinical Microbiology was rightfully referred as a "game changer. In fact, the rapid detection of microorganisms promotes optimal antibiotic use in the face of concerns about resistance, abuse, toxicity, and cost. In addition, this determines a more efficient therapeutic approach and impacts dramatically on the survival of patients, in particular those affected by systemic and severe infections.

4
5 To tackle the growing problem of antimicrobial resistance. Multifaceted interventions are better than single initiatives at reducing the overuse of antibiotics. Proposed actions include a combination of the prohibition of over-the-counter sales of antibiotics, implementation of antimicrobial stewardship programmes, participation of clinicians in audits, use of rapid point-of-care tests, use of delayed antibiotic prescribing strategies, and improved information for patients using information brochures.
6 AntiMicrobial Stewardship: Minimum requirements for developing an institutional programme Creation of a multidisciplinary inter-professional team which optimally should include but is not limited to: an infectious diseases (ID) physician a pharmacist with ID training a clinical microbiologist an infection control professional a hospital epidemiologist

7
8 Why the 24-hour laboratory is an important value in the Hospital? To rapidly manage severe infections (i.e. sepsis) and to reduce mortality To save money reducing the length of stay and the use of antibiotics/antifungals To assess in real-time the local microbial epidemiology of the Hospital and to establish efficacious guidelines for the antimicrobial (empirical) therapy
9 New diagnostic approaches in Clinical Microbiology playing a role in the antimicrobial therapy Mass-spectrometry identification of microorganisms Rapid susceptibility tests (phenotypic, microscopic or molecular) Use of biomarkers for the real-time management of therapies Genomic and/or proteomic approaches for the study of microbiota and genomic characterizations of microorganisms

10
11
12 The GRES (Gestione Rapida Emocolture Sepsi) study Mean time to start antibiotic therapy (SD), days Percentage of effective therapy at the start of antibiotic therapy (SD) Percentage of optimal therapy at the start of antibiotic therapy (SD) Mean duration of antibiotic therapy (SD), days Mean length of hospital stay (SD), days Died at 30 days, n (%) Total N=743 Study period 1 N=197 Study period 2 N=233 Study period 3 N=313 P-value 0.70 (1.4) 0.92 (1.7) 0.71 (1.4) 0.55 (1.1) (18.2) 93.9 (19.0) 91.4 (21.1) 92.6 (15.2) (38.9) 59.0 (42.0) 51.9 (43.0) 71.9 (30.6) < (13.3) 21.9 (15.4) 19.3 (13.3) 17.7 (11.5) (24.5) 29.7 (29.3) 26.8 (24.7) 24.2 (20.7) (15.9) 31 (15.7) 39 (16.7) 48 (15.3) 0.90 Study Period 1: the ID physician was called by a ward physician when patients had positive blood cultures. Study Period 2: the ID physician were called directly by the microbiologist immediately after a pathogen was isolated from blood culture. Study Period 3: the ID physician was called by the microbiologist immediately after a pathogen was identified from the blood culture, and all cases were re-evaluated at bedside 72 h after starting antibiotic therapy in order to optimize therapy Murri et al., Diag. Microbiol. Infect. Dis., 2018
13 Molecular detection of resistance Identification of microbial genes related to drug resistance directly from clinical specimens or from positive blood cultures (to reduce the time-to-result) Reduction of the time to appropriate antibiotic treatment (escalation or de-escalation therapy) Easy to use Relatively few genes included in the proposed panels Expensive (?)
14 Rapid Identification of Escherichia coli and Klebsiella pneumoniae Producing CTX-M and Carbapenemases in Positive Blood Cultures Combined with Bedside Infectious Disease Consultation is Associated with Very Early Initiation of Adequate Antimicrobial Therapy We evaluated the performance and the advantages of a PCR-based rapid detection of bla CTX-M, bla KPC, bla VIM, bla OXA-48 and bla NDM genes (Eazyplex SuperBug CRE) after direct detection of E. coli and/or K. pneumoniae using MALDI BioTyper and/or FilmArray BCID panel. We analyzed 425 cases of bloodstream infections with positive blood cultures (BCs). Resistance genes were detected in 43.5% (191/439) of the isolates with an overall agreement with the culture results of 100%. Total time to identification (median) of the direct method was 18 h (IQR, 8-23 h) versus 46 h (IQR, h) (P<0.001) with the culture-based method. The therapeutic impact of the rapid strategy was evaluated in 327 cases. All these patients received an empirical treatment after BC collection, but it was inadequate in 58.1% of the cases. After real-time communications and bedside infectious disease interventions, 82.1% of the patients with inadequate therapy were switched to an effective coverage at a median time of 20 h (IQR, 10.3 to 25 h) from the starting of diagnostic procedure. Spanu et al, unpublished
15 Positive BC bottle Updated UCSC protocol for the management of positive blood cultures Gram staining Monomicrobial Direct MALDI BioTyper system K. pneumoniae NO Stop Polymicrobial Yes Subculture on solid media FilmArray BCID panel Direct AST Rapidec Carba NP MALDI BioTyper analysis Neg. Result reporting Pos./doubtful Eazyplex Superbug CRE AST Enterobacteriace ae ERT/ MEM MIC > 0.12 µg/ml no Stop Result reporting yes Result reporting Phenotypic and/or molecular tests
16 Class A: presence of blashv, blatem, blactx-m, blaveb, blaper, blages, and/or blakpc Class B: presence of blavim, blaimp, and/or blandm Class C: presence of blaacc, blacmy, bladha, blafox, blamox, and/or blaact Class D: presence of blaoxa-48-like Ceftazidime-Avibactam versus MDR Klebsiella spp.


17 Time Lapse Microscopy


18 Time Lapse Microscopy Piperacillina-Tazobactam Colistina
 and broth microdilution or")
19 This study describe results from a multicenter study evaluating the Accelerate Pheno system. A combination of fresh clinical and seeded blood cultures were tested, and results from the Accelerate Pheno system were compared to Vitek 2 results for identification (ID) and broth microdilution or disk diffusion for AST. Six common Gram-positive cocci and from the 4,142 AST results, the overall essential agreement (EA) and categorical agreement (CA) were 97.6% and 97.9%, respectively. Overall very major error (VME), major error (ME), and minor error (me) rates were 1.0%, 0.7%, and 1.3%, respectively. Eight species of Gram-negative rods were evaluated and from the 6,331 AST results, overall EA and CA were 95.4% and 94.3%, respectively. Overall VME, ME, and me rates were 0.5%, 0.9%, and 4.8%, respectively. On the basis of these results the Accelerate Pheno system seems to be able to identify and provide phenotypic MIC and categorical AST results in a few hours directly from positive blood culture bottles and support accurate antimicrobial adjustment.
20 Performance and diagnostic accuracy of Accelerate ID/AST Blood Culture Assay on clinical blood cultures in the rapid diagnosis of bacteremia The objective of this pilot study was to evaluate the performance of the new Accelerate ID/AST System (Accelerate Diagnostics, Inc.) compared to culture-based method results of positive BCs collected from patients hospitalized at the Fondazione Policlinico Gemelli, Catholic University of the Sacred Heart Medical Center During a 2-week period positive BCs corresponding to unique episodes of BSI were analyzed both by Accelerate ID/AST Blood culture System and standard laboratory testing, which included MALDI-TOF for species identification and microdilution broth for MIC determination A total of 24 episodes of BSIs, including two which were polymicrobial, were included in the study. Overall 26 microorganisms were recovered and the overall species identification agreement was 88.4% (23/26). A total of 132 microorganism-antimicrobial combinations were analysed. Category agreement was 93.2% (123/132). Discrepancies were due to 4 minor errors, 2 major errors and 3 very major errors. False susceptibility emerged exclusively in 3 cases of combination Enterobacteriaceae/piperacillin-tazobactam De Angelis et al., ECCMID 2017
21 Proposed algorithms for use of procalcitonin (PCT) values to determine antibiotic treatment of high-acuity infections (ie, high risk; sepsis) in intensive care unit settings Schuetz et al., Arch. Int. Med., 2011
 to reach a 3 value.")
 did not receive antifungal therapy, whereas 25 (12.6%) were initially treated. In 14 of these 25 patients antifungals were discontinued as negative BDG results were notified.")
22 Objectives: To determine the effects of a strategy that uses (1,3)-β-D-glucan (BDG) results for antifungal treatment of ICU patients at high risk of invasive candidiasis. Methods: Patients were included in the analysis if they exhibited sepsis at the time of BDG testing, and they met Candida-score components (i.e., severe sepsis, total parenteral nutrition, surgery, or multifocal Candida colonization) to reach a 3 value. Results: 198 patients were studied Of 63 BDG-positive patients, 47 with candidemia and 16 with probable Candida infection, all received antifungal therapy Of 135 BDG-negative patients, 110 (55.5%) did not receive antifungal therapy, whereas 25 (12.6%) were initially treated. In 14 of these 25 patients antifungals were discontinued as negative BDG results were notified. Candidemia was subsequently diagnosed only in one patient who did not receive prior antifungal therapy The median antifungal therapy duration in candidemic patients differed from that in noncandidemic patients (14 days [IQR, 6 18 d] vs 4 days [IQR, 3 7 d]; p <0.001) Thus, unnecessary antifungal therapy was avoided in ~73% of potentially treatable patients and it was shortened in another ~20%
.")
, while the reported NPV for candidaemia (also readable as PPV for bacteraemia) was obtained")
23 Positive predictive value (PPV) and negative predictive value (NPV) for candidaemia of (1,3)-β-D-glucan (BDG) and procalcitonin (PCT) considered both separately and in combination (BDG+PCT). The reported PPV for candidaemia (also readable as NPV for bacteraemia) was obtained when both markers were concordant in indicating candidaemia (BDG 80 pg/ml and PCT <2 ng/ml), while the reported NPV for candidaemia (also readable as PPV for bacteraemia) was obtained when both markers when concordant in indicating bacteraemia (BDG <80 pg/ml and PCT 2 ng/ml)
-β-dglucan, mannan, and antimannan serum assays, performed on day 0 and day 4; or to a routine care strategy,")
24 Biomarker strategy for early detection of empirical antifungal therapy Prospective, randomised, controlled single-center unblinded study, performed in a mixed ICU 110 patients were randomly assigned to a strategy in which empirical antifungal treatment duration was determined by (1,3)-β-dglucan, mannan, and antimannan serum assays, performed on day 0 and day 4; or to a routine care strategy, based on international guidelines, which recommend 14 days of treatment Rouze A, et al. Intensive Care Med, 2017
25 Biomarker strategy for early detection of empirical antifungal therapy The primary endpoint of this study was the percentage of patients receiving early discontinuation of empirical antifungal treatment, defined as a discontinuation, for reasons other than death, strictly before day 7 after empirical antifungal treatment initiation. Primary outcome Early discontinuation of empirical antifungal treatment Secondary outcomes Total duration of antifungal treatment Biomarker strategy (n=54) Routine care (n=55) 29 (54) 1 (2) < (4, 13) 13 (12, 14) < No significant difference was found in the percentage of patients with subsequent proven invasive Candida infection, mechanical ventilation-free days, length of ICU stay, cost, and ICU mortality between the two study groups. P Rouze A, et al. Intensive Care Med, 2017
26
27
28 Blood GM testing in diagnosing invasive aspergillosis (ESCMID & ECMM joint recommendations for the laboratory diagnosis of invasive aspergillosis) HRCT: high resolution computed tomography; IA: invasive aspergillosis; ICU: intensive care unit; GM: galactomannan; OD: optical density; PPV: positive predictive value; QoE: quality of evidence; SOT: solid organ tranplantation: SoR: strength of recommendation.. From: Ullmann et al, CMI, 2018
:1696-702.")
29 Effect of anti-mould prophylaxis on serum galactomannan In patients under prophylaxis with mouldactive antifungal drugs GM test should be used as a DIAGNOSTIC TEST and not as a SCREENING TEST!!!! GM: galactomannan. Duarte RF, et al. Clin Infect Dis. 2014;59(12):
 BAL: bronchoalveolar lavage; CSF: cerebrospinal fluid; GM: galactomannan; QoE: quality of evidence; SoR: strength of recommendation.")
30 GM testing in diagnosing invasive aspergillosis in other clinical samples (ESCMID & ECMM joint recommendations for the laboratory diagnosis of invasive aspergillosis) BAL: bronchoalveolar lavage; CSF: cerebrospinal fluid; GM: galactomannan; QoE: quality of evidence; SoR: strength of recommendation. From: Ullmann et al, CMI, 2018

31 T2Candida Panel powered by T2 Magnetic Resonance (T2MR) T2MR combines proven magnetic resonance with innovative nanotechnology to accurately identify Candida pathogens in whole blood faster and easier than blood culture-based diagnostics. T2Candida is cleared by the US FDA and EMA for the diagnosis of candidemia. Pfaller et al., Future Microbiol, 2016
32 T2Candida was devised to not amplify freely circulating, non-cell-associated DNA. Using primers for ribosomal DNA intervening transcribed spacer region 2, results are reported as positive or negative for C. albicans/c. tropicalis, C. glabrata/c. krusei, and C. parapsilosis >1500 control patients with Candida-negative blood cultures 6 patients with Candida-positive blood cultures 250 contrived blood samples spiked with C. albicans/c. tropicalis, C. glabrata/c. krusei, and C. parapsilosis T2Candida identified 98.1% of patients as noncandidemic, with a mean time to negative result of 4.2 ± 0.9 hours. The overall sensitivity per patient (excluding invalid results) was found to be 91.1%, with a mean time to positive result of 4.4 ± 1.0 hours The limit of detection was 1 3 cfu/ml (1 cfu/ml for C. tropicalis and C. krusei, 2 cfu/ml for C. albicans and C. glabrata, and 3 cfu/ml for C. parapsilosis)
33 Assuming sensitivity of 90% and specificity of 98%, anticipated positive and negative predictive values (PPVs/NPVs) of T2Candida can be calculated Thus, T2Candida performance characteristics enable clinicians to assign clinical settings in which T2Candida is most likely to be useful in guiding antifungal treatment decisions. Indeed, PPVs may exceed a threshold that justifies antifungal treatment, while corresponding NPVs render active candidemia extremely unlikely.

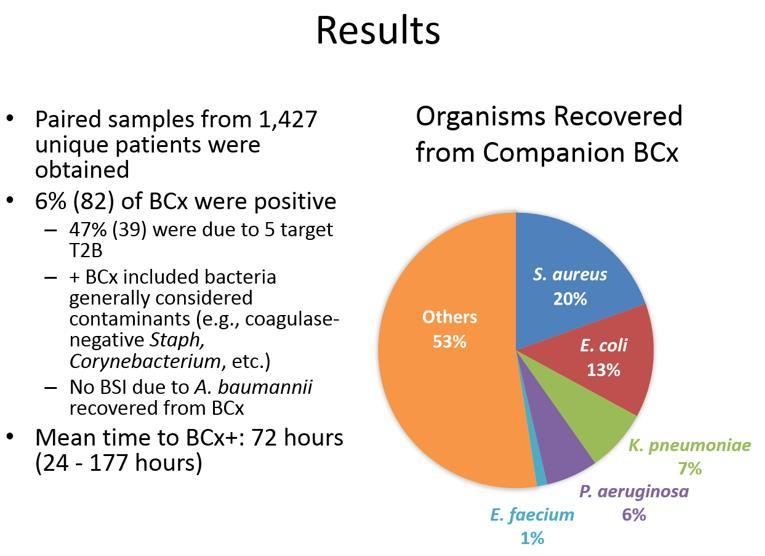
34 Performance of T2Bacteria Panel for rapid identification of bacteria responsible of bloodstream infections Positive results more than 4.5 times faster: Positive results for a bacterial infection with T2Bacteria were available in 5.5 hours, compared to a mean time of 25 hours for blood culture. Every hour of providing targeted therapy to patients faster can reduce patient mortality rates by 7.6%. Negative results 20 times faster: A negative result took 120 hours (5 days) for blood culture, compared to 6.1 hours with the T2Bacteria Panel. Excellent accuracy: The T2Bacteria Panel had 89.5% sensitivity and 98.4% specificity in comparison with clinical criterion of a true infection. The authors point out that blood culture-based diagnostics have a sensitivity as low as 65% for the first blood culture draw. Potential impact on therapy: The authors found that 66.7% of the clinically infected patients missed by blood culture and correctly identified by T2Bacteria were being inappropriately treated at the time of the T2Bacteria result. De Angelis et al., JAC, 2018
35 Performance of the T2Bacteria Panel in clinical blood samples according to Clinical Infection used as the gold standard assessed by detection channel De Angelis et al., JAC, 2018

36
37

38


39
40 Thirteen different genes were detected from 38 patients, including the ermb gene (40.8%), the bla OXA-51 -like gene (28.6%), the sul1 (28.6%) and int1 (20.4%) integrase genes, and the meca and bla CTX-M genes (12.3% each). Detection of resistance genes influenced modification of therapy in all 15 cases with multiple MDR bacteria. In 3 of these patients, Unyvero and culture identified MDR pathogens with good correlations between phenotype and genotype for antimicrobial resistance, leading to modification in antibiotic regimes to appropriate therapy. Thirteen (86.7%) of these 15 patients improved clinically and bacteriologically and 2 (13.3%) died, mainly from their comorbidities. Ten (66.7%) would have been inappropriately treated if treatment had been based on results of conventional testing or empirical therapy only.

41 Host response biomarkers: a new way to discriminate between sepsis and SIRS? Positive Correlation between SeptiScore and the Probability of Sepsis. In each panel the probability of sepsis is plotted against SeptiScore for four different SeptiScore ranges.
42 Conclusions More than ever, it is emphasized the primary role of a clinical microbiology laboratory, that is to assist clinicians in the diagnosis and treatment of infectious diseases, and to support infection control specialists in their tasks. In many instances, however, the delay between the collection of the specimen and the results of the microbial culture makes the latter unhelpful for the clinician. Therefore, advances in diagnostic methods (such as POC or POC-like tests) and/or procedures might satisfy the need for speed, particularly when clinicians, infection control specialists, and microbiologists confront with a septic patient or, in general, with a patient with a systemic infection, or deal with an emerging epidemic.