Contents. 1. Background 2. Introduction to the manual 3. Purpose 4. The Monitoring System. Annexes:
|
|
|
- Jocelyn Hart
- 5 years ago
- Views:
Transcription

1
2
3
4
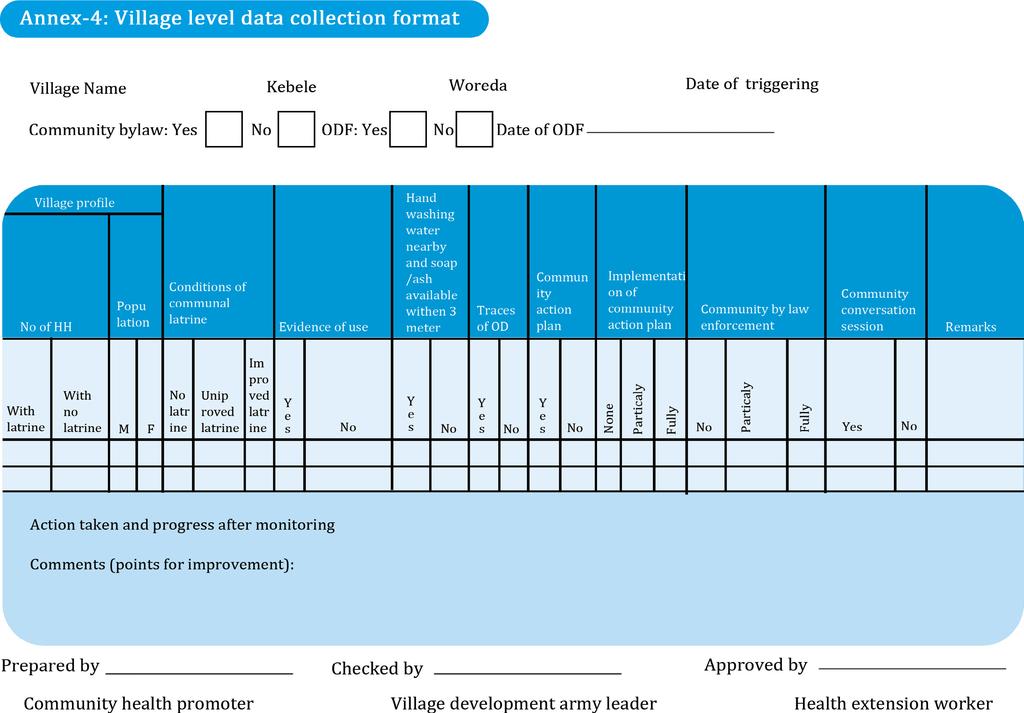
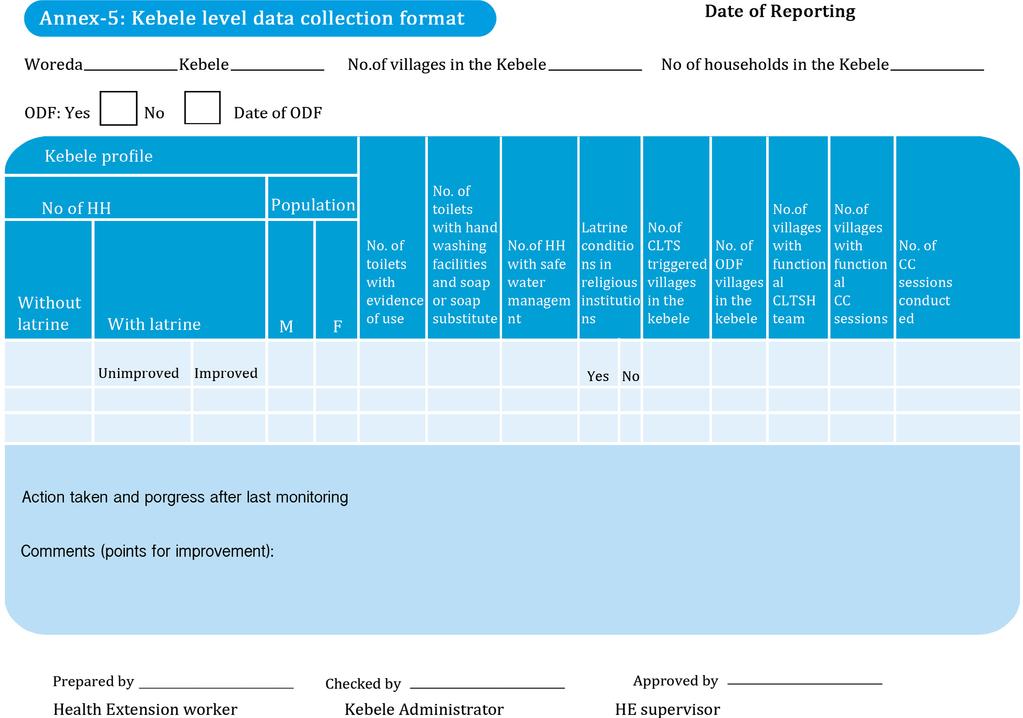
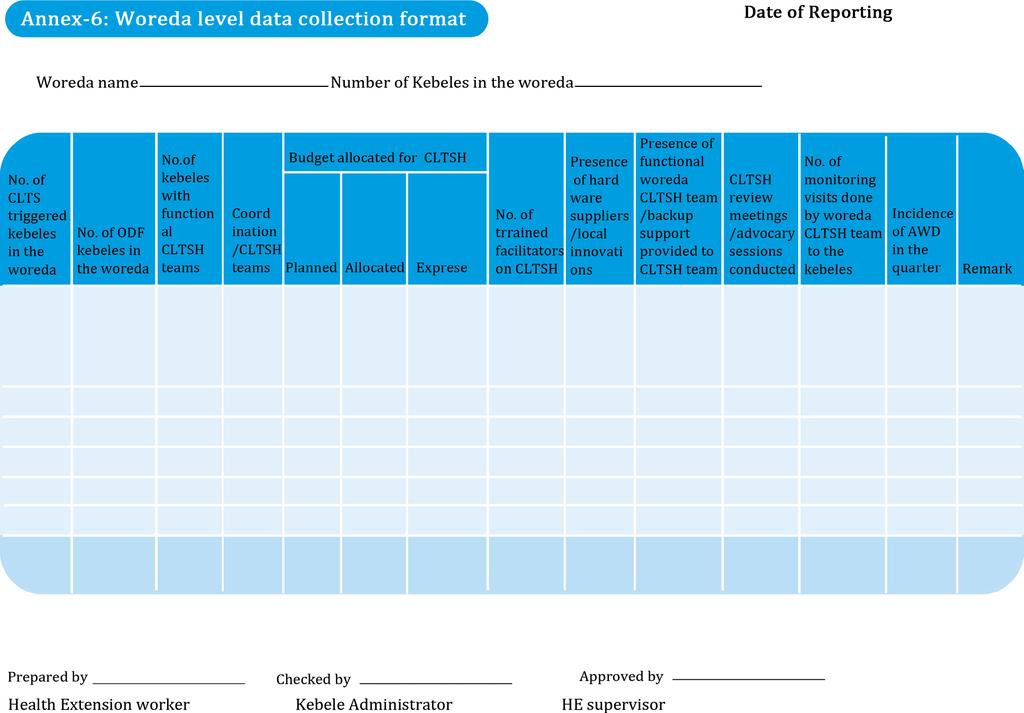
5 Contents 1. Background 2. Introduction to the manual 3. Purpose 4. The Monitoring System 4.1. What to Monitor 4.2. Data Source 4.3. How to Monitor/ Data collection method 4.4. Frequency of Monitoring 4.5. Who is Responsible for Monitoring? 4.6 Reflecting Critically to Improve action 5. Reporting/Communication 5.1. Reporting Channel (who to report to) 5.2. What Information do Stakeholders Need? 5.3. Stakeholder Composition and Responsibility Village CLTSH comittee/team Kebele WASH team composition and responsibilities Woreda WASH team composition and responsibilities Regional/Zone WASH team composition and responsibilities Federal Level stakeholdres and responsibilities 6. Frequency and flow of reporting 7. The data management system Annexes: Annex-1: Data Monitoring Templates for Implementation of Community-Led Total Sanitation and Hygiene Annex-2: School Data Collection Format Annex-3: Health Institutes Data Collection Format Annex-4: Village Level Data Collection Format Annex-5: Kebele Level Data Collection Format Annex-6: Woreda Level Data Collection Format
6
7 1. Background Inadequate water supply and sanitation services are still the major cause of children death and sickness in Ethiopia, Infant Mortality Rate (IMR) is 77/1000, under five mortality rates is 123/1000. Significant number suffers from regular bouts of diarrhoea or parasitic worm infection that ruins their life. Women and children are the main victims. They must also endure the indignity, shame and sickness that results from the lack of hygienic sanitation. The impact of deficient water supply and sanitation services falls primarily on the poor. Their poverty is aggravated and their productivity is impaired, while their sickness puts severe strains on health services and hospital. Apart from these there is also a powerful environmental reason to improve sanitation and hygiene services for the poor. Human waste is a major polluter of rivers and groundwater resources. Scarcity of water is a major consideration where water resources have to be protected and conserved. Coverage levels for water and sanitation in Ethiopia are still low even after a considerable effort is provided by the government and other support organizations. The sanitation coverage as officially reported by the ministry is 60%. In general, there are low levels of hygiene awareness, which compound the health risks associated with low water and sanitation coverage levels. The main problem is increased susceptibility to water-borne diseases such as diarrhoea and dysentery, water-washed diseases such as trachoma and scabies, water-based diseases such as schistosomiasis, and water-rrelated insect vectors including malaria. In Ethiopia, almost three quarters of health problems in children and communicable diseases originate from the environment. Diarrhoeal disease alone accounts for 17 per cent of total under-five mortality. In addition to diarrhoeal disease, a large section of the population is afflicted with trachoma and helminthiasis, especially guinea-worm disease. This is evidenced by frequent outbreaks of water related epidemics in both rural and urban areas. Low levels of water and sanitation coverage also have important social implications. Women and children spend several hours every day fetching water. For girls, the task of carrying water combined with lack of sanitary facilities in schools often stands in the way of their education. To address this government of Ethiopia is implementing a 20 year health sector development program (HSDP) divided in to 3-5 year rolling plans. In 2003 during HSDP II an innovative community based program, health extension program (HEP) was introduced. The objective of HEP is to improve equitable access to preventive essential health services through community (Kebele) based health services with strong focus on sustained preventive health actions and increased health awareness. As parts of increased level of commitment towards hygiene and environmental health services policies such as the National Sanitation Strategy is developed in 2006 that is enabling framework and serve to motivate and align relevant actors to speed up sanitation coverage and hygiene behavioural change. It places greater emphasis on on-site hygiene and sanitation. The primary focus is on blocking faeces from entering the living environment through the safe management of faeces, hand washing at critical times and the safe water chain from source to mouth. It places responsibility for improving on-site household hygiene and sanitation firmly in the hands of the household with the direct support of the health extension worker and other resources at community level. The strategy is harmonised with the Health Sector Development Programme which places a strong focus on high impact, broad reach, and public health interventions.
8
9 2. Introduction to the manual The key idea in this manual is to use monitoring to help manage the resources and activities of CLTSH intervention to enhance impact along a continuum, from short term to long term. This requires in clarity about the desired goals like open defecation free status. This helps to understand if lower level outputs are contributing to higher level outcomes amidst other influencing factors. It also requires conscious effort to learn to identify corrective actions that could further enhance impact. Keeping track of the detail of CLTSH implementation and gathering good information about what has been achieved are very important. But in the end what makes the real difference is how community members are motivated and supported to learn and contribute to the best of their ability. Monitoring helps to empower the community by creating opportunity to reflect critically on CLTSH intervention and make their own judgments about its value and decide on improvements. It is the people involved in CLTSH intervention who will make it succeed or fail. Their participation in learning how to improve it throughout its existence is vital. Monitoring being an open and critically reflective communication process facilitates participatory learning process. As CLTSH gives more space to grass root institutes, its monitoring enhances meaningful participation. It requires both data on CLTSH activities and personal accounts of people s experience. Therefore participatory monitoring provides opportunities for people with relevant views about the CLTSH intervention to learn how to improve it. Generally this manual supports the monitoring of CLTSH intervention which will strengthen its management by Providing health extension workers and health extension supervisors with information they need for day to day decisions Providing Federal and regional health sector practitioners with the information needed to guide CLTSH intervention towards achieving its goal and objectives Provide early warning of problematic activities and processes that need corrective action Build understanding and capacity amongst those involved in CLTSH intervention Motivate and stimulate learning amongst those committed to making the CLTSH intervention a success Assess progress and so enable accountability requirements to be met. Existing experiences in a number of regions and from different actors show that one of a serious limitation in CLTS implementation in so far is absence of dependable monitoring system to ensure its effectiveness. It is also a challenge that different actors use different approaches to ensure its effectiveness. It is also a challenge that different actors use different approaches to monitor their CLTS intervention. Hence there is a need to develop and harmonize a good monitoring system to support the management of CLTSH intervention. This manual therefore serves the different level actors of health sector to guide CLTSH implementation by Clarifying what observable changes are expected and how that can be achieved Deciding how progress and impact will be monitored Planning how collecting and analyzing the necessary information for tracking progress and impact Explain the reason for success and failure and agree on how to use this understanding to improve future action 1
10 3. Purpose The purpose of this monitoring, reporting and data management manual is to standardize the process of compiling, managing and disseminating CLTSH related information at all levels. This manual seeks to provide a set of tools that can be used for tracking progress in CLTSH implementation and for reporting achievements. It is designed to respect resource limitations by allowing for hardcopy data collection at local level. From the woreda up to the federal level, it offers a simple but robust software system for information management. 4. The Monitoring System To best inform decision making, document best practices and advocate for long-term behavioural change, performance must be monitored systematically from the moment implementation gets underway. The core of the process is to compare actual performance against planned targets. The key elements to be monitored are implementation of planned activities against schedule, achievement of expected results, and disbursement of funds against the allocated budget. Setting up the monitoring system can start by identifying the information need (what to monitor) that is detailed by performance indicators, then you need to decide where to find this information that is followed by planning how to collect and analyse this information. Agreeing on the data collection frequency, who will be responsible to do it and planning how stakeholders reflect critically based on the collected and analysed information makes the monitoring system operational What to Monitor Performance questions, information needs and indicators To get to where you want to go, you need to know what information to seek to guide the journey. If you don t ask the right question you will not get useful answers hence knowing what you need to know i.e. selecting good indicator for which you will need to collect data is critical. before CLTSH is triggered helps provide a baseline for comparison and for determining realistic planned targets. Sanitation and hygiene baseline data including household and institutional data, village sanitation maps, and information about existing or potential defecation sites, provides a basis for comparison throughout the monitoring process. The common approach to establish monitoring indicators is to consider each objective level in the objective hierarchy from the log frame and start listing corresponding indicators. Working with performance questions to guide indicator analysis will give a more integrated and meaningful picture of overall CLTSH achievements. Performance questions are not just about what has been achieved. They also ask why there is success or failure and what has been learned to improve future action. Some of the CLTSH intervention performance indicators which need to be monitored are; number of triggered villages, number of ODF villages and causes of success and failure stories. 2

11 Baseline Monitoring involves repeated assessments of a situation over time. Having an initial basis for comparison helps to assess what has changed over a period of time and if this is the result of interventions presence. Information on sanitation and hygiene levels collected in the period before CLTSH is triggered helps provide a baseline for comparison and for determining realistic planned targets. Sanitation and hygiene baseline data including household and institutional data, village sanitation maps, and information about existing or potential defecation sites, provides a basis for comparison throughout the monitoring process Data Source CLTSH progress data can be found in households, villages, and community level institutes. The impressions of field staff such as health extension workers and health supervisors including the feeling of the target people are important sources of information How to monitor/ Data collection method A participatory approach to monitoring is crucial to securing ownership and fostering sustained behavioral change. It is a bottom-up system, beginning at the level of households and proceeding up through to the national level. Participatory monitoring employs various instruments, including the following: CLTS pre-triggering (pre-activation) baseline information review Focus group/community discussions (qualitative data on behavioral change) Key informant interviews/inquiries/community conversations Rapid assessment and field observations (potential defecation sites around water points, forests and bushes, roadsides, funeral places, churches and mosques) Data collection (households, village, schools and health institutions) Multi-stakeholder meetings/forums 4.4. Frequency of monitoring The frequency of monitoring varies with the level of operation from community to federal ministry. Table-1: Key actors and frequency of monitoring 3

12 4.5. Who is Responsible for Monitoring From an institutional perspective, the responsibility for monitoring CLTSH lies with the health sector as a whole, at all levels; Federal, regional, zonal, woreda, kebele and community level. Community based institutions and individuals themselves are also involved in the monitoring chain. Monitoring teams are structured cascading the health sector from village level volunteers up to the Federal ministry. Although the actual team composition may vary from site to site the following members are recommended; Table-2: Monitoring team composition and key tasks 4



13 4.6 Reflecting critically to improve action Critical reflection means interpreting experiences and data to create new insights and agreements on action. After asking what is happening through the collected information it is important to reflect on Why is that happening? What is the implication for the intervention? and What to do next? Finally developing the necessary data collection form to collect data will facilitate the conditions to make the system work. Table-3: Performance monitoring framework Apart from results performance it is also important to monitor operational information to know if we are making optimal use of resources and that operations are of good quality. This provides information how CLTSH service is being delivered by the sector from Federal Ministry up to woreda level structure. 5


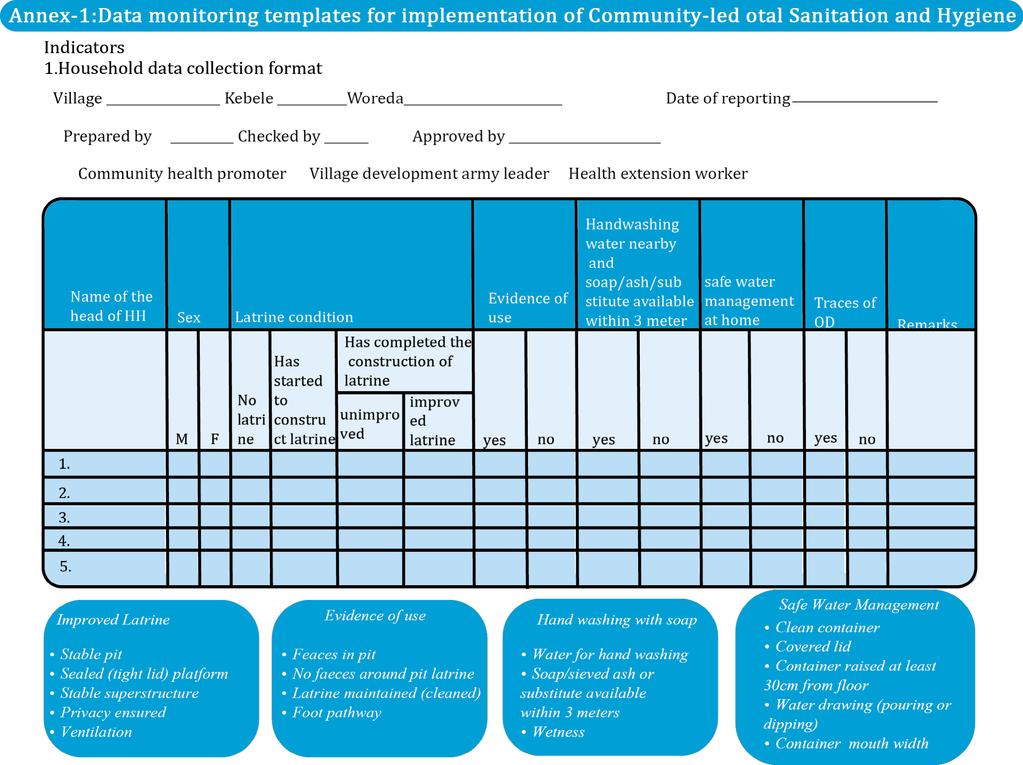
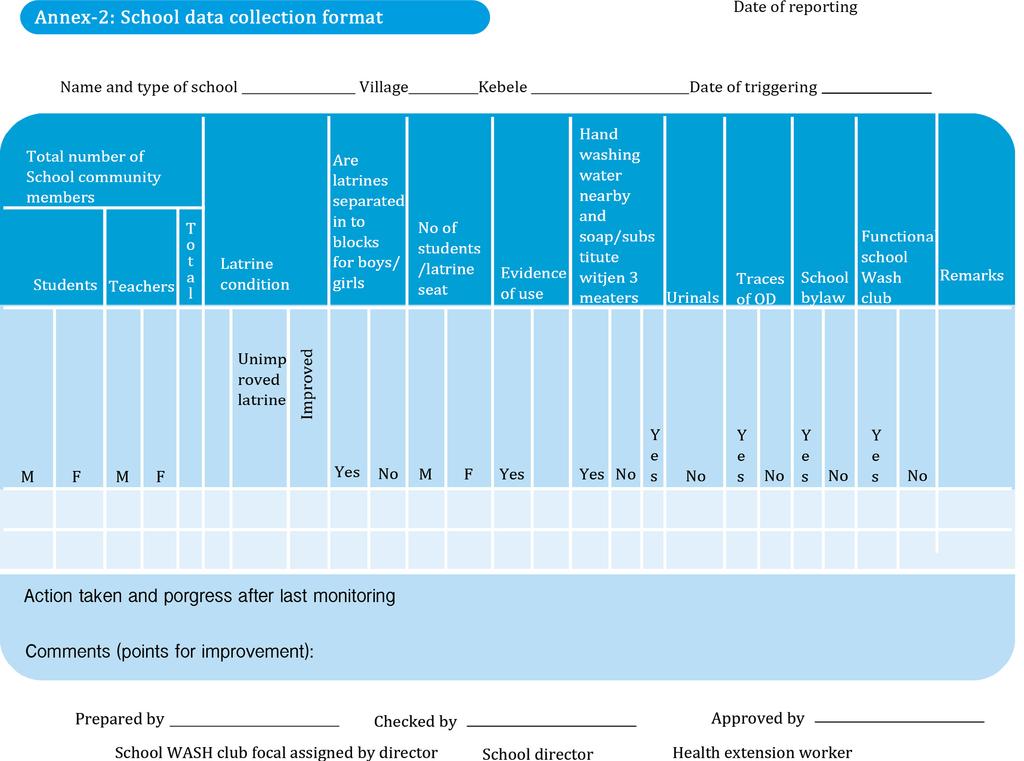
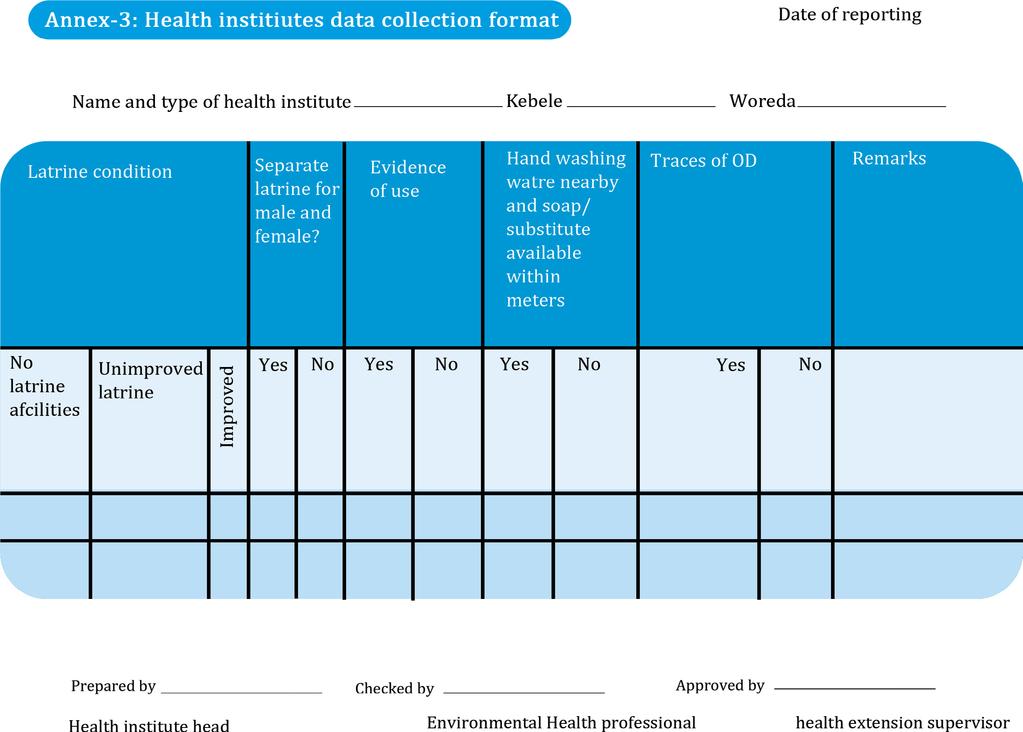
14 Table-4: Implementation monitoring framework Monitoring templates that have been developed based on national WASH inventory formats were prepared with reference to this framework. These are included as annexes at the end of this booklet. 5. Reporting/Communication The results of monitoring must be reported to two groups of partners thus are; 1. mplementing partners at operational level such as from community to woreda level actors for the purpose of reacting on initial findings for its accuracy, reach on joint conclu sion and agree on the next steps and 2. greed findings will be reported to regional and federal level health sector, funding agencies and cooperating institutes to fulfil accountability needs and for advocacy purposes. With this regard the kebele CLTSH team is accountable to the woreda WASH team and required to report to the team on a monthly basis. To report effectively, monitoring teams must know how to report (that is, the reporting format), to whom they are reporting, what they are reporting on, and when to report (Table-5). 6
15 7
16 8
17 Kebele WASH team composition and responsibilities Led by heath extension workers and kebele administrators, the kebele WASH team includes the kebele manager, school directors, development agents, women and youth associations, and natural leaders individuals who are naturally gifted with strong leadership abilities. Team members work together to do the following: Guided by the CLTSH Community action plan, support the implementation and monitor ing of CLTSH programs by assisting with the collection of data and by helping to facilitate discussion and analysis of changes that are happening as the village progress towards achieving CLTSH goals. Advocate for an open defecation free (ODF) environment and associated public health benefits Woreda WASH team composition and responsibilities The woreda WASH monitoring/reporting team is made up of woreda administrators and heads of woreda health, water, education and finance offices. Coordinators from the national Health Extension Program, education cluster supervisors, and other partners (NGOs) provide the team with technical guidance. Guided by the CLTSH Kebele Action Plan, support the implementation and monitoring of CLTSH programs by assisting with the collection of data and by helping to facilitate discus sion and analysis of kebele-level progress toward CLTSH goals. Advocate for an open defecation free (ODF) environment and associated public health benefits Regional/Zone WASH team composition and responsibilities These have similar structre with that of the woreda WASH team compostion i.e. they are lead by Region and zone health sectors as being a lead for the CLTSH process. They will by mandate guide and support the respective woreda level structure. They are supposed to provide finacial, professional and capacity building supports to the woreda level actors They are also expected to demand the woreda level performance and provide a solution for any problem found in the program implemenattaion Federal Level stakeholdres and responsibilities The ministry of health takes the lead in steering country wide CLTSH implementation while other ministries collaborate towards its effective rolling out. Donors, CSOs and other stakeholders will team up with the effort to bring about the realization of CLSTH intervention towards in bringing the require sanitation and hygiene improvement that lead to reduced societal disease burden. 9

18 6. Frequency and flow of reporting 10
19 11
20 12
21 13
22 14
23 15
24 16
25 17
26