CAP Regulatory Potpourri for Microbiologists. Christi Wojewoda, MD Director of Clinical Microbiology 2/2/19
|
|
|
- Christal Gaines
- 5 years ago
- Views:
Transcription

1 CAP Regulatory Potpourri for Microbiologists Christi Wojewoda, MD Director of Clinical Microbiology 2/2/19
2 Disclosures Vice Chair of the CAP Microbiology Committee Immediate Past Vice Chair of the CAP Continuous Compliance Committee State Commissioner for CAP for Vermont, New Hampshire and Western Massachusetts Very CAP heavy talk! 2
3 Objectives Chose the most appropriate PT products for your lab s test menu. Review updated microbiology CAP checklist requirements. Understand what has been learned from IQCP implementation. 3
4 PT Terminology Regulated analytes 83 regulated analytes 5 regulated subspecialties PT is required and monitored by CMS Non-regulated analytes For all other analytes, PT performance is not monitored by CMS CFR (c) requires that the laboratory verify the accuracy of any tests not included on the list of regulated analytes at least twice per year June
5 Proficiency Testing Requirements - Regulated Microbiology Five Microbiology Subspecialties Bacteriology Mycology Mycobacteriology* Parasitology Virology Criteria for evaluation described in CLIA regulations 5 challenges 3 times per year 5
6 Proficiency Testing Requirements - Non-regulated analytes CAP requires enrollment in a CAP-Accepted PT program for many non-regulated analytes The Continuous Compliance Committee of the CAP determines which non-regulated analytes should require enrollment in a CAP-accepted PT program Determination based on: Clinical relevance/significance of analytes Availability of graded PT Examples of Micro required, but not regulated analytes would be Trichomonas antigen, H pylori urease, and HIV viral load 6
7 What is a required analyte? CAP term that includes all regulated analytes and many non-regulated analytes (both waived and non-waived) Laboratories with a required analyte on their activity menu MUST enroll in a CAP-accepted PT Program for that analyte CAP accreditation program only monitors/sends compliance notices for required analytes 7
8 How to figure out what PT is required? AKA why is this so confusing? Master Activity Menu with PT Options (in e-lab Solutions Suite). Laboratory s Activity Menu (in e-lab Solutions Suite). (COM The laboratory s current CAP activity menu should accurately reflect the testing performed) Analyte/Procedure Index of the Surveys Catalog (on ). 8
9 Master Activity Menu with PT Options 9
10 Master Activity Menu with PT options June
11 Laboratory s Activity Menu June

12 Analyte/Procedure Index of Surveys Catalog 12

13 PT catalog 13

14 Laboratory s Activity Menu June
15 Bacteriology PT requirements C. Diff could be satisfied with D survey June

16 C diff, continued June


17 Why does best fit matter? Lab originally enrolled in D4 Activity menu listed Bacterial ID, urine and throat culture Switched to MC5 which provides more challenges and is a better fit to cover sample sources the lab is testing. June

18 Best fit in Parasitology Lab originally enrolled in P Activity menu changed to drop blood parasite ID, so needed to switch to P4, otherwise would not have enough samples to satisfy CLIA June

19 Virology PT issue For the subspecialty of virology, a lab was only performing qualitative molecular HSV They were enrolled in ID1 survey o Does not satisfy CMS requirements Need to enroll in a 5x3 for HSV 19
20 If PT is not required, what do you need to do for APA? Best practice would be to participate in and evaluate commercial PT if available If not available or you select not to: o Have a Procedure to document plan o Establish evaluation criteria/acceptability limits o Document performance at least semi-annually o Test samples that span the clinically relevant range o Use patient samples o Test enough samples o Evaluate trends o Corrective action for each unacceptable result o CLSI GP29-A2. Assessment of Laboratory Tests When Proficiency Testing Is Not Available June
21 PT pitfalls One of the most common reasons for getting a PT result incorrect in Micro is reporting beyond the level of how you would report a patient Have records available to prove you are reporting to the level of patient results June

22 2017 Top Ten Checklist Deficiencies - Overall


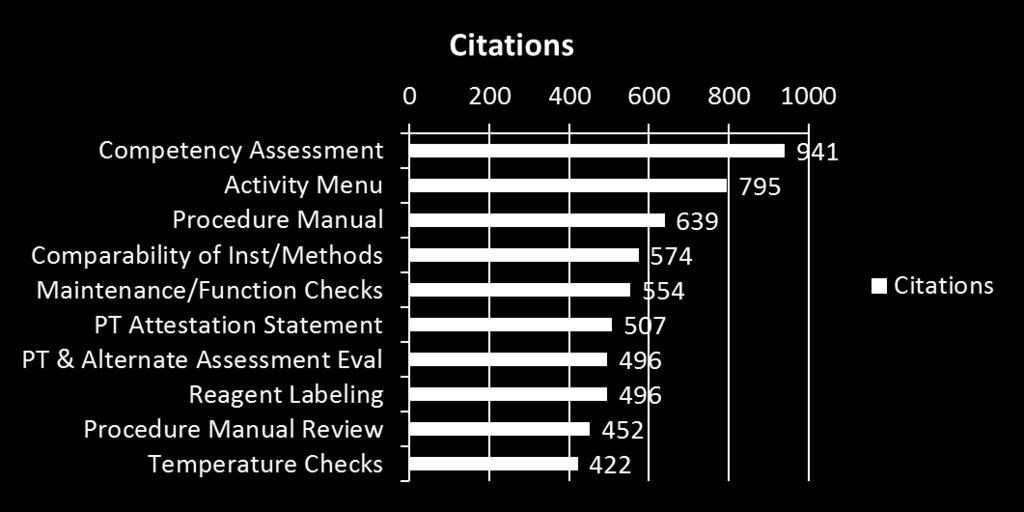
23 2017 Top Ten Checklist Deficiencies - Microbiology
24 GEN Competency Assessment The competency of personnel performing nonwaived testing is assessed at the required frequency at the laboratory (CAP/CLIA number) where testing is performed. All test performance variations must be included in the competency assessment specific to the site or laboratory. Records of competency assessment may be maintained centrally within a healthcare system but must be available upon request. Separate requirement for waived testing (GEN.55499). Revised in 8/21/17 checklist edition
25 Competency Assessment - continued During the first year of an individual s duties, competency must be assessed at least semiannually and annually thereafter. Prior to performing patient testing, training must be completed and evaluated for proper test performance. Training and competency assessments are separate processes. Applicable to new testing personnel only and not for existing testing personnel trained on new test methods.
26 Competency Assessment - continued Assessment includes all applicable six elements of competency noted under GEN for each test system. Use laboratory activity menu to identify test systems. Same analyte with two test systems (e.g. automated, manual) needs separate competency assessments. Multiple analytes under single test system do not need separate competency assessments (e.g. chemistry panel). Each test system includes assessment of preanalytic, analytic, and postanalytic steps in the testing process.
27 Competency Assessment - continued Individuals responsible for competency assessments have the education and experience to evaluate the complexity of testing being assessed (GEN.55510). High complexity testing: section director (technical supervisor) or individual meeting general supervisor qualifications Minimum qualifications: Associate degree in laboratory science or medical technology with at least two years of training/experience in high complexity testing Moderate complexity testing: Technical consultant or individual meeting those qualifications Minimum qualifications: Bachelor s degree in a chemical, physical, biological or clinical laboratory science of medical technology from an accredited institution with at least two years of training and/or experience in nonwaived testing
28 Competency: Written Procedure Detailed procedure that reflects the process Who can perform assessment Frequency of assessment How six elements are utilized How assessment is recorded/documented How new testing is incorporated Retraining and reassessment process when problems identified
29 Competency Assessment Records Create a grid Define test systems Component steps of the test system Element(s) used to assess Date assessment performed Person performing assessment

30 Microbiology Competency Example 29 January
31 COM Activity Menu Procedure manual should correspond to Activity Menu Add to new test implementation process Audit Activity Menu periodically at the section/department level, especially when doing reapplication Remove retired tests Custom checklist is generated by Activity Menu selections Inaccurate activity menu may result in a non-routine inspection and added expense for the laboratory. Most commonly identified at the routine onsite inspection Inspection team may not have expertise in some specialty areas. Insufficient time to inspect additional testing such as multiple POCT areas. Checklists or checklist requirements may not be available to the inspection team applicable to the additional testing.
32 COM Procedure Manual Written procedure must match the laboratory s practice Electronic manuals must be available to all personnel, and must have down time alternative Reviews must be biennial (every two years) by medical director or designee and must be recorded Schedule in document control 3 months prior to due date Single signature on manual s table of contents is not sufficient Procedures must be available for inspector
33 Procedure Manual - continued Following a change in laboratory directorship, the new laboratory director approves the laboratory policies and procedures over a reasonable period of time (TLC.11485). The approval must be recorded. Format is at the discretion of the laboratory director and include an itemization of the documents reviewed/approved, signatures/dates. Approval should be completed within three months of the directorship change.
34 COM Comparability of Instruments and Methods Specific to Microbiology Non-waived methods only Methods within a single CAP/CLIA number At least twice a year Applies to two instruments used to detect the same analyte Two or more detectors connected to a single data collection computer before going to the LIS are considered one instrument Written procedures including acceptance criteria Patient samples, controls
35 Comparability of Instruments/Methods cont. List the instruments to be compared Designate the time frame for the study Identify who will perform the study Indicate the specimens to be used for study Specify the data to be collected Specify how to analyze the data Establish acceptability criteria (COM.04300) Document review of data, actions taken
36 COM PT Attestation Statement The proficiency testing attestation statement is signed by the laboratory director or designee and all individuals involved in the testing process. Physical signatures must be present. PT results submitted electronically can have printed names but will require the physical signatures on the original attestation page. Electronic signatures are not acceptable.
37 COM.1400 PT Attestation - continued Designees must be qualified through education and experience to meet the defined regulatory requirements associated with the complexity of testing. High complexity technical supervisor or section director Transfusion service medical director/section director (technical supervisor) must be an MD or DO Moderate complexity technical consultant
38 COM Proficiency Testing Evaluation Each unacceptable PT or alternate assessment result (any result or sample not meeting defined acceptability criteria) must be evaluated. Investigate each unacceptable PT result for impact on patient sample results. Major categories of investigation include: Clerical; Analytical; Procedural; Specimen handling; PT material Correction of problems appropriate to the failure are performed in a timely manner.
39 MIC Monthly QC Review Most common MIC deficiency Review must include documentation of corrective action Review must be timely 29 January
40 MIC Blood Culture Volume For blood cultures on adults Optimum volume should be monitored Frequency of monitoring may be determined by the laboratory Method may be determined by the laboratory (eg weight or lines on the bottle) Provide feedback to the clinical staff of inadequate volumes 29 January
41 MIC Morphologic Observation Assessment Intent to ensure consistency among staff Include Gram, trichrome and other organism stains Best practice is to use circulation of patient slides Must include assessment 29 January
42 MIC Selection of Antimicrobial Agents to Report Written policies to ensure agents appropriate for the organism and body site Policies must be reviewed with the stakeholders annually if the laboratory is part of a health institution and records of review should be available ( s, meeting minutes, etc.) Same policies should be used when reporting proficiency testing 29 January
43 Summary: Avoiding the Most Common Deficiencies Written procedure for what you are doing. Document that shows that you are doing it. Review QM monitors for improvement Cross reference checklist item with documentation. Anticipate inspector requests and think like an inspector!
44 IQCP: Lessons Learned From On-Site CAP Inspections Approximately 1500 deficiencies were cited in 2016 related to IQCP (55% All Common & 44% discipline specific checklists) In 2017, there were 1203 deficiencies cited (67% All Common & 33% discipline specific checklists) June 7, 2018
 55 Hematology 5 Microbiology 228 Point of Care 56 1203 June 7,")
45 Overall IQCP Citations for 2017 Requirement (ID) 2017 Citations All Common 802 Chemistry 57 Limited Service (not micro) 55 Hematology 5 Microbiology 228 Point of Care June 7, 2018


46 Microbiology Citations June 7, 2018
47 2017 Deficiency Data The most common reasons for lacking an IQCP: Laboratories misunderstood the complexity of testing performed Especially related to kit testing for Micro IQCP implemented after the January 1, 2016 deadline Microbiology laboratories continued to follow CLSI guidelines for media, ID, and/or susceptibility without implementing an IQCP Keep in mind that an IQCP is not required but default QC must be followed if there is no IQCP June 7, 2018
48 Default QC - Micro Default QC refers to quality control as defined in CLIA 88 Two levels of external control per day of patient testing for most tests Applies to Direct Antigen Testing (non-waived) Applies to Molecular Testing Platforms Media QC Each new lot/shipment sterility, selectivity, biochemical characteristics, growth ( includes blood culture media) June 7, 2018
49 Default QC - continued Identification systems Each new lot/shipment demonstrate positive and negative reactivity for each substrate Antimicrobial Susceptibility Testing (AST) Daily with all appropriate organisms June 7, 2018
50 Benefits of IQCP Based on the analysis of a risk assessment for a test system May allow for the reduction of quality control DAT and Molecular with internal controls rely on the internal control for daily QC Media use the exempt/non-exempt rules from CLSI but must include sterility for the nonexempt ID systems streamlined QC using fewer organisms AST weekly QC June 7, 2018
51 IQCP Development Tips 19% of the All Common microbiology deficiencies were for inadequate risk assessment Use a template that lists all five of the risk assessment factors Reagents, environment, specimen, test personnel, test system Use a consistent template throughout your laboratory Rate the risks by severity and likelihood of occurrence Address all risks that are determined to be unacceptable June 7, 2018
52 Risk Assessment (RA) Risk assessment includes all of the following: Preanalytic, analytic, and postanalytic phases of the testing process Components of the tests including all five factors Data from the laboratory s own environment/instrument/testing personnel, showing acceptable performance over the maximum time interval between external quality control runs Intended medical uses of the test and impact if inaccurate results are reported (clinical risk) Manufacturer s instructions and recommendations The IQCP cannot have QC frequency less than the manufacturer requires June 7, 2018
53 Inspector Observations Historical QC is used as part of the risk assessment, but there is no time frame of the exact period assessed or raw data available. Risk assessment will state historical data evaluated and no errors or corrective actions recorded. If no time frame specified cannot determine if data was evaluated for the necessary time period. June 7, 2018
54 Quality Control Plan (QC) The individualized quality control plan must define all aspects monitored based on the potential errors identified during the risk assessment, including the following parameters as applicable: The number, type (external and internal quality control systems), and frequency of quality control Criteria for acceptable performance Monitoring of the testing environment and reagents Specimen quality Instrument calibration, maintenance, and function checks Training and competency of testing personnel June 7, 2018
55 Example Monthly QC Review Form June 7, 2018
56 Quality Assessment (QA) Ongoing quality assessment monitoring records for QC, instrument/equipment maintenance and function checks, complaints, errors, and corrective actions. COM.50600: Quality Assurance Monitoring Added a new statement based on CMS input: o Re-evaluation of the quality control plan if changes to the reagents, environment, specimen, testing personnel, or test system elements of the risk assessment occur. An example form for annual QA assessment of the IQCP is available on CAP.org (IQCP resources page) June 7, 2018
57 Annual Assessment of IQCP June 7, 2018
58 Annual Assessment Page Two June 7, 2018
59 Common Participant Questions If my laboratory (satellite lab) does microbiology culture set up and blood culture collection and sends the cultures to an affiliated laboratory for testing, do we need an IQCP for the media involved? If media is received from the laboratory that will be performing the testing, the satellite lab is not responsible for the end user quality control of the media. The reference laboratory is responsible for media QC or use of an IQCP. The satellite lab is responsible for a visual examination of the media (MIC.21420) upon receipt and may also have an IQCP for the extent of their handling of the media. Any laboratory that receives media directly from the manufacturer is responsible for media QC or use of an IQCP (MIC.21240, MIC.21420) regardless of whether culture testing is performed or referred. If any culture result, such as findings of No growth, are reported by the satellite laboratory, it is responsible for media QC or use of an IQCP, regardless of whether it receives the media directly from the manufacturer or from another laboratory. June 7, 2018
60 Participant Questions - continued If an instrument or device is used to perform multiple tests, is a separate IQCP required for each test? Is it okay to use the same IQCP for different tests on the Cepheid? Many of the same risks will apply to all tests performed on an instrument or device; however, risks may vary for specific tests. The risk assessment performed must address all potential areas of risk for each test, as well as the instrument or device. Based on the outcome of the risk assessment, a single IQCP may or may not be appropriate for the instrument or device. June 7, 2018
61 Participant Questions - continued Can I add an additional test performed on the same instrument or an additional test site onto an existing IQCP? Yes, providing the following actions should are taken: Review and modify the existing risk assessment to ensure that risks specific to the new test or test site have been properly evaluated for each of the five components of IQCP (reagents, environment, specimen, test system, testing personnel) and the three phases of testing. Evaluate laboratory-specific data (historical or new) relating to the modification and include a summary of the evaluation with the risk assessment. Obtain laboratory director approval of the modifications to the quality control plan. Retain records of the risk assessment and changes to the quality control plan. Ensure that appropriate ongoing quality assessment processes are in place for the added test or testing site. Update the laboratory s List of Individualized Quality Control Plans form for inspection readiness. June 7, 2018
62 Participant Questions - continued AST If you receive a new susceptibility panel or a new instrument (same model) what is required for your IQCP? A new panel and/or a new instrument must be verified good reference is the CLSI M52 Reference to CLSI criteria must be included in your IQCP After verification, review the risk assessment for changes, make any necessary changes to the IQCP and have your laboratory director sign the revised IQCP June 7, 2018

63 Questions 63