Centralized GME What Can Your GME Office Do For You? B15, Part B Jaclyn Goodfellow & Kathryn MacRae
|
|
|
- Clement Lawrence
- 5 years ago
- Views:
Transcription
1 Centralized GME What Can Your GME Office Do For You? B15, Part B Jaclyn Goodfellow & Kathryn MacRae
2 Disclosure No conflicts of interest to report





3 Grand Rapids Medical Education Partners Introduction and Background Consortium Model: Spectrum Health, Mercy Health St. Mary s, Michigan State University-College of Human Medicine, Grand Valley State University 19 ACGME Accredited Programs 16 Program Coordinators 305 Residents & Fellows Developed in 2000 with the merger of two community teaching hospitals ALL Residents and staff are employees of the consortium
4 Central GME Office Supported By Director of Accreditation and Compliance GME Coordinator Manager GME Scheduling and Projects Manager Scheduling Assistant GME Project Specialist GME Coordinator (2) Also supported by Finance Department HR Department Education Services Research Department
5 Program Coordinator Manager All Program Coordinators report to central GME Manager Dedicated manager rather than management tasks added to the GME Director role Program Director is not the employer, however: Input given for PC performance evaluations Provide work direction PDs are not employees of GRMEP Provides connection between programs and central office
6 Why Centralization? New and extra requirements from NAS Created added pressures and work requirements for coordinators Efficiencies for staff and residents Provides oversight of tasks for uniform implementation Meets legal and institutional requirements







7 Developing Central Tasks Centralization Committee Participants 5 Program Coordinators (representing 4 different programs) Coordinator Manager GME Directors HR Director to facilitate
8 Developing Central Tasks Representatives from other departments were also invited Education Services Human Resources Finance CME All suggestions were vetted with appropriate departments Implementation determined by: Tasks providing immediate time savings across programs Tasks minimizing legal risk
9 Implementation Examples ADS review and best practice sharing Visas Difficult to keep up to date with changing requirements and needs; moved to HR Verifications Very time consuming, especially in the spring/summer as graduates became credentialed; moved to HR Resident Reimbursement Central office distributes pre-loaded credit cards with education stipend (allocated by programs). Tracking usage and reimbursement requests became cumbersome; process moved to central GME Meal Card Tracking
10 Implementation Examples Scheduling After the merger in 2000 we developed a city-wide master scheduling process All programs and learners, both GRMEP AND non-grmep, are required to schedule experiences through the central GME office Placements, requests, and vetting Schedule parameters Any rotation changes (approximately 180 per block) Approximately 1200 total learners 305 Residents/Fellows 158 Visiting Residents/Fellows 375 MSU/CHM Medical Students (1-4) 134 PA Students 118 NP Students 175 Visiting Students Notifies all departments of learners on service before each new block HIM, security, medical group leadership, programs and coordinators, IT, educators, clinic managers etc.



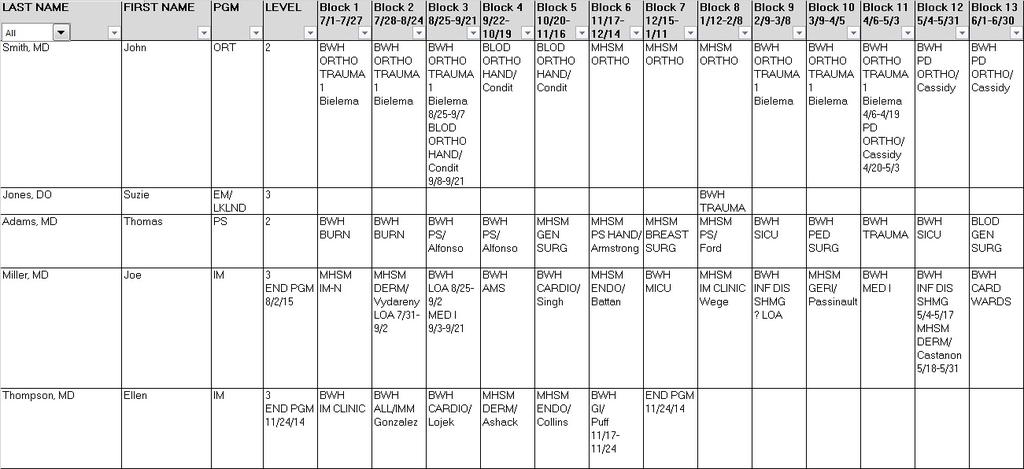
11 Implementation Examples Example of the GRMEP Master Schedule
12 Implementation Examples Resident/Fellow Onboarding and Orientation Scheduled by GME office personnel Collects required documents: Diplomas Faculty appointment for Michigan State University Certification Cards License application Lab Coat orders IRIS requirements and training gap information





13 Implementation Examples
14 Implementation Examples Curriculum Support Increased need in this area due to Milestones and NAS requirements Dedicated education content developer works with programs to establish updated curriculum


15
16 Additional Implementation Items: Certification Card tracking (upload to RMS) Compliance tracking moved to HR Flu, TB, and respirator fit tests Recruitment Support Corporate hotel discounts Direct Billing from restaurants Promotional materials Applicant lodging reimbursements Coordination of recruitment fair participation Post-match Communication Residency Management System Super Users Workshops and education during PC meetings Faculty and CCC development Core Conferences Developed and tracked by GME for all interns Topics include: Physician impairment Medical ethics Research support GME finance
17 Additional Implementation Items: Contracts Organized and tracked by one GME Coordinator Licensing and Step 3 Applications and renewals coordinated and tracked by one GME Coordinator Call Schedules Central upload of schedules to new hospital communication system Duty Hours GME Coordinator runs RMS violation reports Cleans up violations Distributes to each program to investigate true violations; programs report back to GMEC quarterly










18 Successes and Barriers Successes Time saved in programs Participative leadership boosted morale Easier and earlier identification of potential program issues Coverage for leaves and absences Barriers Resistance to Change (PC and PD) Centralization Committee helped with buy-in Offense taken when suggestions given Meeting each program s unique needs Need for process improvement after implementation




19 Where Are We Now? Reallocation of staff Central GME and within programs Centralization committee continues to meet and work on process improvement
20 Any Questions? Contact us: