2016 Europe-Nordic-US Symposium New Frontiers in Antibacterial Resistance Research. Pharmacological Approaches to Address AR
|
|
|
- Jasper Hall
- 5 years ago
- Views:
Transcription
1 2016 Europe-Nordic-US Symposium New Frontiers in Antibacterial Resistance Research Pharmacological Approaches to Address AR G.L. Drusano, M.D. Professor and Director Institute for Therapeutic Innovation University of Florida The vast bulk of the data presented here was supported by multiple R01 s from NIAID
2 Pharmacological Approaches to Address Antimicrobial Resistance What will we look at? 1. Impact of the intensity of drug exposure on bacterial cell kill and resistance emergence 2. Impact of duration of therapy on resistance emergence 3. Combination chemotherapy
3 Cell Kill and Resistance Emergence Impact of Intensity of Drug Exposure

4 Cell Kill and Resistance Suppression in Pseudomonas aeruginosa
5 Cell Kill and Resistance Suppression in Pseudomonas aeruginosa Bacterial burden at therapy initiation < inverse of the mutational frequency to resistance Bacterial burden at therapy initiation > inverse of the mutational frequency to resistance Jumbe et al J Clin Invest 2003;112:
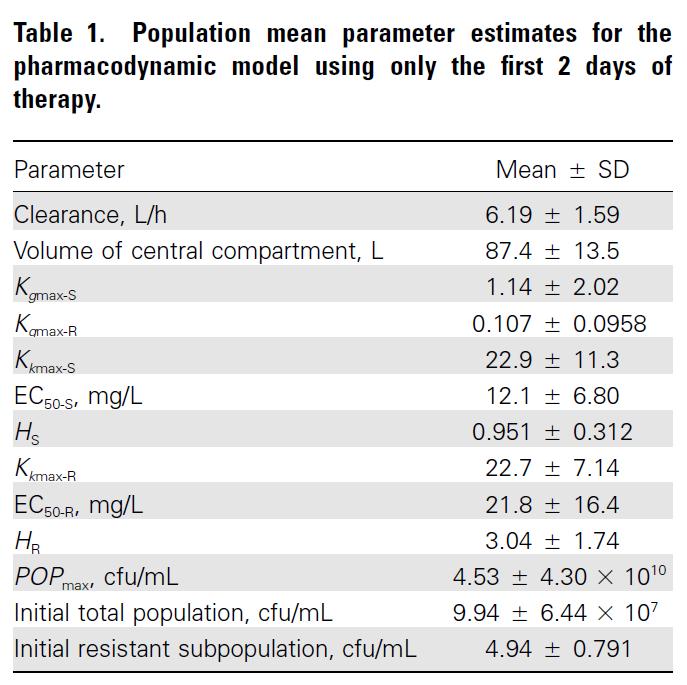
6 Peripheral (thigh) Compartment (C p ) + Bacteria (X T/R ) k cp k pc f(c) IP injection Central Blood Compartment (C c ) PD dx S =K GS x X S x L - f KS (C c H ) x X S dt dx R = K GR x X R x L- f KR (C c H ) x X R dt [4] [5] PK k e L = (1- (X R + X S )/POPMAX) [6] [1] [2] [3] dc a = -k a C a dt dc c = k a C a +k pc Cp-k cp C c -k e C c dt dc p = k cp C c - k pc C p dt f (C c H )= Y 1 =X T =X S +X R Y 2 =X R K max C c H C H 50 +C c H, =K and = S,R [7] [8] [9]
7 Cell Kill and Resistance Suppression in Pseudomonas aeruginosa
8 Cell Kill and Resistance Suppression in Pseudomonas aeruginosa Prospective Validation Experiment Lines are NOT best-fit lines AUC/MIC = 52 AUC/MIC = 157 They are prospective prediction lines about which the data have been scattered Journal of Clinical Investigation 2003;112: & Nature Reviews Microbiology 2004;2:
9
10 Resistance Suppression in Pseudomonas aeruginosa The use of the hollow fiber model for studying antimicrobial regimens was described by Blaser and Zinner and employed extensively by Dudley
11 Resistance Suppression in Pseudomonas aeruginosa = Total Bacterial Burden; = Less-Susceptible Bacterial Burden Tam V et al. Bacterial-population responses to drug selective pressure: Examination of garenoxacin s effect on Pseudomonas aeruginosa. J Infect Dis 2005;192:
12 Prospective Validation Experiment Predictions: 1. AUC/MIC = 137 gives good cell kill then fails due to resistance 2. AUC/MIC =200 gives good cell kill and suppresses resistance
13 Cell Kill and Resistance Suppression in Pseudomonas aeruginosa Why has it taken a while to get a handle on resistance suppression by dosing? We are used to looking for relationships that are monotonic give more drug; obtain more exposure; drive better effect The functional form for resistance suppression is NON-MONOTONIC!
14 Resistant Mutants (CFU/mL) Cell Kill and Resistance Suppression in Pseudomonas aeruginosa Cell Kill Monotonic Function Resistance Suppression Non-Monotonic Function It s easier to kill than suppress amplification of resistant clones Resistant organisms at baseline AUC 0-24 :MIC Ratio All other data points represent resistant organism counts at 48 hours of therapy
15 Patient Translation: Does the resistancesuppression target and Monte Carlo Simulation reflect clinical outcomes? Taking the expectation demonstrates an overall target attainment of 62% and a predicted emergence of resistance rate of 38%
16 Resistance Suppression in Pseudomonas aeruginosa Is Monte Carlo Simulation Predictive? Peloquin studied 200 mg IV Q 12 h of ciprofloxacin in nosocomial pneumonia - P aeruginosa resistance rate 70% (7/10 - pneumonia only) - 77% (10/13 - pneumonia plus empyema [2] and bronchiectasis [1]) Monte Carlo simulation with a resistance suppression target (AUC/MIC = 157) predicts suppression in 24.8% Fink et al studied ciprofloxacin in nosocomial pneumonia at a dose of 400 mg IV Q 8 h - P aeruginosa resistance rate 33% (12/36) Monte Carlo simulation at this dose predicts resistance in 38.2% Peloquin et al Arch Int Med 1989; Fink et al AAC 1994;38:547-57
17 Pharmacological Approaches to Address AR What are the take-home messages? 1. Resistance suppression is non-monotonic i.e. follows an inverted U 2. Intermediate exposures actually amplify lesssusceptible sub-populations
18 Pharmacological Approaches to Address AR What are the take-home messages (cont d)? 3. The size of the bacterial burden is critical as it increases the probability of a primary mutant being present at baseline 4. Identifying a resistance suppression threshold of exposure is not enough use Monte Carlo simulation to see how many in a population will attain the suppression threshold
19 Impact of Therapy Duration

20
21
22 Total Bacterial Burden Prospective Validation Experiment Predictions: 1. AUC/MIC = 100 suppresses for 5 days, then fails 2. AUC/MIC =280 suppresses for at least 10 days Less-Susceptible Bacterial Burden
23 Pharmacological Approaches to Address AR What are the take-home messages? 1. The longer therapy goes, the harder it is to suppress amplification of less-susceptible populations 2. An inadequate regimen that is administered for too long a time may result in complete obliteration of the susceptible population this population will never return at this point even when drug pressure is stopped
24 Pharmacological Approaches to Address AR Looking at Agents in Combination

25 Mono-Rx Pseudomonas aeruginosa
26 Cefepime vs P. aeruginosa So, what s going on? Why the failure of mono-rx and why the success of combo-rx? AAC 2012; 56:
27 Impact of Baseline Bacterial Burden So, what is going on? We looked at the stability of cefepime over time at different baseline inocula Inoculum and timedependent hydrolysis was seen Hypothesis: β-lactamase mediated problem Antimicrob Agents Chemother 2012;56:
28 It is Probably the β-lactamase! No resistance emergence!
29 Success of Combination Therapy It Is the β-lactamase! As a protein synthesis inhibitor, we hypothesize that the aminoglycoside shuts down the expression of the ampc β-lactamase These results were recapitulated with qpcr as the readout Sometimes combination therapy has a salutary outcome and it is not just due to synergistic cell kill! AAC 2012; 56:
30

31
32 Pharmacological Approaches to Address AR What are the take-home messages? 1. Again, the bacterial burden makes a difference! Think why VABP is so hard to treat 2. Sometimes, you simply can t get there from here with monotherapy
33 Pharmacological Approaches to Address AR What are the take-home messages (cont d)? 3. Combination therapy is NOT simple and straightforward, but properly chosen can help ameliorate some of our problems
34 Pharmacological Approaches to Address AR: Conclusions We can have a significant impact on resistance emergence if we pay attention to dosing The duration of therapy makes a difference This is a fine balance long enough to cure the patient; short enough to suppress resistance Sometimes you just need combination therapy Where? Serious infections with large bacterial burdens e.g. VABP; especially non-fermentors Regulatory authorities need to think out of the box on this (Drs. Powell and Cavaleri of EMA get it)
35 Thank You for Your Attention! For those with any interest (at all) in this topic, it has recently been reviewed: 1. Drusano GL, A Louie, A MacGowan, and W Hope. Suppression of Emergence of Resistance in Pathogenic Bacteria: Keeping our Powder Dry-Part 1. Accepted. Antimicrob Agents Chemother. 2. Drusano GL, W. Hope, A MacGowan, A Louie. Suppression of Emergence of Resistance in Pathogenic Bacteria: Keeping our Powder Dry-Part 2.Accepted. Antimicrob Agents Chemother. Contact info for George Drusano: gdrusano@ufl.edu; (407) ; (518) (mobile)
36 BACK UP SLIDES
37
38
39

40 Cell Kill and Resistance Suppression in Pseudomonas aeruginosa Jumbe et al J Clin Invest 2003;112: & Drusano GL. Nat Rev Microbiol 2004;2:
41 Central + Bacteria Infusion Compartment (C c ) (X T/R ) SCl f(c) [1] dc c =Infusion-(SCl/V)xC c dt dx S =K GS x X S x L - f KS (C c H ) x X S dt dx R = K GR x X R x L- f KR (C c H ) x X R dt [2] [3] L = (1-(X R + X S )/POPMAX) [4] f (C c H )= K max C c H C H 50 +C c H, =K and = S,R [5] Y 1 =X T =X S +X R, IC(1)=1.01x10 8 Y 2 =X R, IC(2)= 58 [6] [7]
42

43

44
45
46
47 Combination Therapy for Resistance Suppression We have gone as long as 6 months; 1-2 months is standard for us in MTB studies
48 Combination Therapy for Resistance Suppression The model system has 5 outputs There are 5 inhomogeneous differential equations Dimensionality is 28 Drug interaction is quantitated through a variation of the Greco model Anyone wishing to go over the enabling equations can talk with me offline

49 Combination Therapy for Resistance Suppression Fully Susceptible Linezolid-S; Rif-R Rif-S; Linezolid-R
50 Combination Therapy for Resistance Suppression The model system allows Monte Carlo simulation to be performed This tells us what a fixed regimen will do in a large patient population Here circa half the patients will have the susceptible population wiped out with all 508/1000 patients left with only resistant isolates