! Background. ! What is really new?! The new Section 7: Explorative Clinical Trials (ECTs) ! Consequences in General
|
|
|
- Richard Hopkins
- 5 years ago
- Views:
Transcription
1 ! Background! What is really new?! The new Section 7: Explorative Clinical Trials (ECTs)! 5 Approaches (Table 3) for:! Microdose trials (7.1)! Single-Dose (SD) Trials at Sub-therapeutic Doses or Into the Anticipated Therapeutic Range (7.2)! Multiple-Dose (MD) Trials (7.3)! Consequences in General! Consequences Based on Previous Experience! Chances and Limitations of ECTs! Consequences for Study Planning! Conclusions 1
2 ! The 1 st scope of ALL regulatory guidance for early drug development is SAFETY of the study participants. Minimizing risk implicates (besides product quality): 1) Pre-clinical data MUST be sufficient. 2) Number of participants MUST be as low as possible. 3) The starting dose(s) and dose increments MUST be safe. " Maximum tolerated dose is beyond the scope of M3(R2) 4) Dosing within a dose group may need to be staggered.! ALL Phase-0/I studies are of explorative nature: Nevertheless, the limited no. of participants should give reliable information on 1) Safety and tolerability 2) Pharmacokinetics (PK)! The revised M3(R2) guidance summarize and extend previous guidance focused on: 3) Pharmacodynamics (PD) and efficacy! BUT: There is NO therapeutic / diagnostic intention. 2
3 ! The revised M3(R2) guidance shall allow " To speed up the selection of the most appropriate drug candidate (out of 2 or more) based on early human data " To accelerate Go/No go decisions ( frontload ) " To avoid late stage attrition rates for candidate drugs, a major problem for industry, patients and authorities " To assist in development of MORE drugs! by means of EARLY use of (translational) biomarkers for characterization of human PD / efficacy! The new M3/(R2) guidance incorporates / superseeds / extends: " Previous M3 versions (CDER 1995 / EMEA 2000) " Jun 2004: CPMP/SWP/2599/02/Rev. 1 Position Paper on Non-clinical Safety Studies to Support Clinical Trials With a Single Microdose " Jan 2006: CDER Guidance for Industry, Investigators, and Reviewers. Exploratory IND Studies " Jun 2006: EMEA/CHMP/SWP/91850/2006 Concept paper on the development of a CHMP guideline on the non-clinical requirements to support early phase I clinical trials with pharmaceutical compounds 3
4 ! The new M3/(R2) guidance does NOT address: " Additional guidance to traditional Phase-I/II studies " Development of biologics (timing only!) " Decision-making for dosing by: Human equivalent dose (HED) or Minimum anticipated biological effect level (MABEL) " Decision-making for maximum doses in Phase-I/II! Other Phase-I guidance still need to be considered, if ECT trials do not appear to be useful / appropriate " Advantage cannot be used (e.g. indication, methods) " Biomarkers not available / not informative 4
5 Section to be addressed in this talk: 7. EXPLORATORY CLINICAL TRIALS 7.1 Microdose trials " 2 approaches (1 & 2) 7.2 SD trials at sub-therapeutic doses or into the anticipated therapeutic range " 1 approach (3) 7.3 Multiple dose trials " 2 approaches (4 & 5)! Usefulness in comparison to traditional Phase I/II? Besides Sections: 13. Immunotoxicity 14. Photosafety Testing 15. Nonclinical Abuse Liability 16. Other Toxicity Studies 17. Combination Drug Toxicity Testing 5
6 App. 1: Single (or divided) dose(s) microdose study - Total exposure: #100 µg AND 1/100 NOAEL/active dose App. 2: Multiple (#5) dose(s) #100 µg microdose study - Total exposure: #500 µg AND 1/100 NOAEL/active dose per dose AND washout of $6 x t1/2 (actual/predicted) App. 3: Single dose: sub-therapeutic to therapeutic range - Doses based on extended SD toxicity: rodent+non-rodent App. 4: Multiple-dose study #14 days # therap. range only - Doses based on 2-week toxicity: rodent+non-rodent App. 5: Multiple-dose study #14 days # therap. range only - Similar to 4 with slightly different pre-clinical requirements Posology from actual / predicted exposure: oral [mg/m 2 ] ; i.v. [mg/kg] App. 1/2 total exposure: SD #100 µg / MD #500 µg App. 3: SD FiH study " Exposure: extended SD toxicity - Starting dose: Not exactly defined, dependent on MSS - Maximum dose: #1/2 NOAEL in MSS " IF toxicity is monitorable AND reversible in man App. 4: MD FiH study " See differences in species tox.! - Starting dose: 1/10 or 1/50 of NOAEL AUC in MSS - Maximum dose: < NOAEL in MSS or 1/2 AUC App. 5: MD FiH study " Follow OR to be agreed with CA - Starting dose: 1/50 in MSS - Maximum dose: # 1/2 NOAEL AUC in rodent OR # NOAEL AUC in non-rodent MSS, most sensitivity species; CA, competent (regional) authority 6
7 For ALL approaches stated:! In vitro target/receptor profiling should be conducted! Appropriate characterization of primary pharmacology (mode of action and/or effects) in a pharmacodynamically relevant model should be available to support human dose selection. App. 1 & 2: No core battery of safety pharmacology* App. 3: Core battery of safety pharmacology* App. 4 & 5: Core battery of safety pharmacology* " doses similar to those used for the toxicity studies *, The core battery includes in accordance with ICH S7A and S7B: effects on cardiovascular, central nervous, and respiratory systems, and should generally be conducted before human exposure. App. 1: Extended single dose toxicity " Footnote c: Specification for identical toxicity for App. 2 " Footnote d: Reversibility on Day 14; dose $ 100x the clinical dose App. 2: 7-day repeated-dose toxicity " Hematology, clin. chemistry, necropsy and histopathology required Identical for App. 1 & 2: " Toxicity study usually in rodent by intended route of administration (or I.v.) with toxicokinetic data. A maximum dose of 1000-fold the clinical dose (mg/kg for i.v. / mg/m 2 for oral) can be used. App. 3-5: Rodent AND non-rodent toxicity required 7
8 App. 3: Extended single dose toxicity " Intended clinical route of administration " Top dose should be MTD, MFD or limit dose App. 4: 2-week repeated-dose toxicity " Standard parameters in rodents + non-rodents " Doses in animals based on exposure multiples of anticipated clinical AUC at maximum dose App. 5: Standard 2-week repeated-dose toxicity " Primary study in rodents (justification!) " Top dose should be MTD, MFD or limit dose " Confirmatory study $3 days +X in non-rodent (n=3)* Alternative: escalating dose study in non-rodent* $3 days + X *, at the anticipated NOAEL exposure in rodent ; X = clinical study duration MTD, Maximum Tolerated Dose MFD, Maximum Feasible Dose App. 1 & 2: None recommended " But studies or SAR* assessments to be included in the CTA " For highly radioactive agents: appropriate PK and dosimetry App. 3 to 5: Ames assay or alternative (identical) " If Ames is inappropriate (e.g. antibacterial products) App. 4: PLUS an assay (in vitro or in vivo) capable of: " Detecting chromosomal damage in a mammalian system App. 5: As App. 4 PLUS (in case of in vivo assessment): " This could be part of the rodent toxicity study *, SAR: structure-activity relationship 8
9 Risk identified for an (Exploratory) Clinical Trial? YES NO CHMP/SWP/28367/07 Guideline on strategies to identify and mitigate risks for FiH trials ICH M3 (R2) Nonclinical Safety Studies for the Conduct of Human Clinical Trials MABEL, then: Microdosing or NOAEL Microdosing or NOAEL then MABEL 9
10 Molecular Markers Biochemical Markers Functional Markers Structural Markers Genomics Proteomics Biochemistry Metabolomics Functional Changes Tissue Changes Minutes Hours Hours Days Days Months Days Months Preclinical Evaluation Plasma concentrations? Validated* biomarker(s) available? Target modulation predictive for humans? Target modulation at predictive for humans? Target modulation at safe plasma levels? Human Study PK PD O.K. O.K. % 1 % 2 O.K. % 2 % 1 O.K.??? 1??? 2 % 1??? 2??? 1 % 2 Likely Decision GO NO GO NO GO GO/NO GO? GO/NO GO? GO/NO GO? NO GO *, Validation should be 1, PK formulation appropriate? known best BEFORE, 2, PD appropriate? otherwise development Multimodal PD necessary? 10

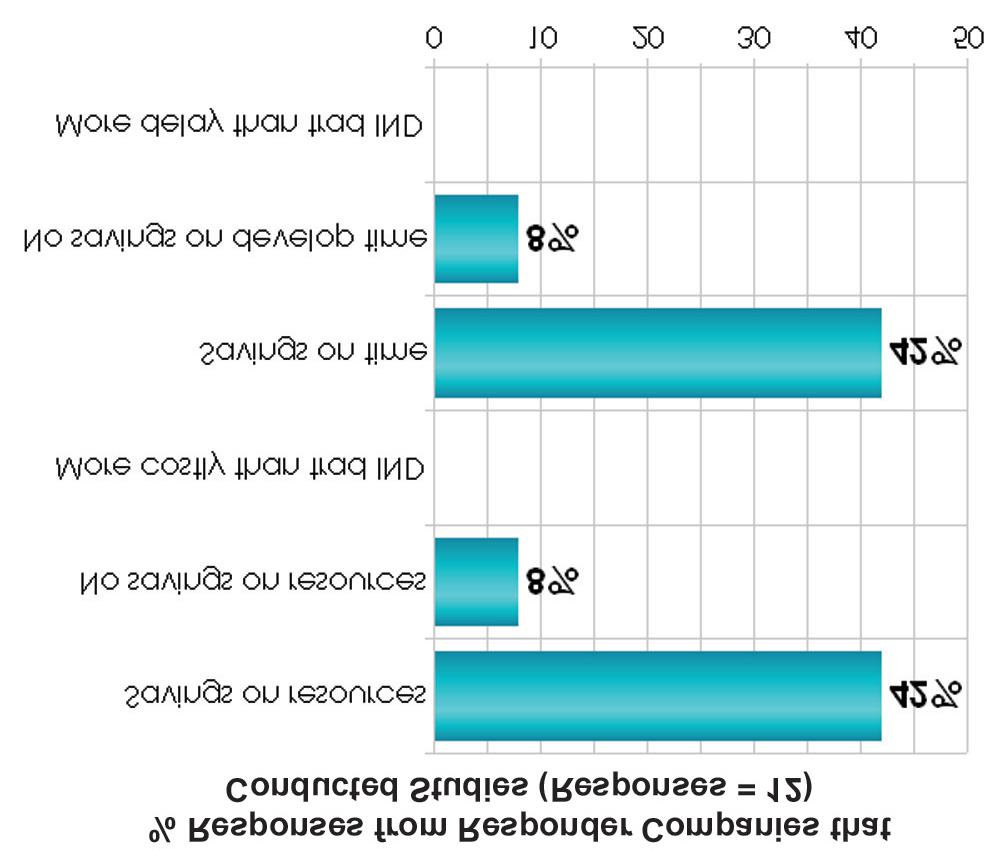
 for ECTs are")
11 Unfortunately: NO recent examples are available to demonstrate any progress intended by the new regulation Thus: Experience from previous microdose and expind regulation is referred to And: Future perspectives on Clinical Trial Applications (CTAs) for ECTs are provided. 11

12 12
13 13
14 General: " Safety problems OR PD may not be evident at too low doses " Willingness of severely ill patients for non-therapeutic trials, if PD is not assessable in healthy volunteers? For an unsuccessful candidate all approaches may lead to: " Saving of animals " Early withdrawal (risk of error!) of not promising candidates " Saving of time & costs For a successful candidate all approaches may lead to: " Additional pre-clinical studies and animals " Additional clinical studies (critical for rare diseases: multicenter!) " Early decision as promising candidate with a risk of later withdrawal " Additional time & costs Advantages of Microdose Approaches 1 & 2 (n<15): " Particularly useful, where no animal model reflects PD (e.g., Alzheimer, HIV) " PET study, in particular for CNS imaging " Other biomarkers, e.g. biopsies can be useful for App. 1 & 2 " Selection of lead candidate (out of 2-5 compounds) SD-PK parallel-group design (often n= 4-6) " SD PK bioavailability, t 1/2 for dosing schedule OR 2-way crossover (n=4-6), i.v. vs. other routes OR exclusion of systemic exposure (SD or MD) " PK interaction on candidate, crossover study (n=4-6) " No full GMP quality necessary 14
15 Drawbacks: " Accelerator mass spectrometry (AMS) is time & cost intensive " Generation of an appropriate 14 C tracer is time & cost intensive " Erroneous PK results in 3/10 cases (Oosterhuis, Bioanalysis 2010; 2: 377-9) vs. successful in >80% (Lappin & Garner, Expert Opin Drug Metab Toxicol 2008;4: ) " Possible safety problems may not be evident at too low doses. " Appropriate biomarker may not be available! Future solution by practice : Trend to shift to App. 3 (or intermediate of App. 1 & 3)? App. 3 (or intermediate of 1 and 3) could save most time & costs for candidates / studies regarding: " PK up to relevant doses using cheaper & faster MS/MS methods incl. drug-drug / food-drug interactions " Safety up to therapeutic doses often preferable vs. microdoses " PD may save costs & time (if assessable with single doses), e.g., for glucose, cholesterol or surrogate PK for antibacterials " (Bayesian) PK, PK-PD modeling may be useful for predictions Drawbacks: " Do GMP requirements will still be a major hurdle for ECTs? " Healthy subjects directly followed by patients are not foreseen 15
16 Advantages of Approaches 4 & 5 regarding: " PK up to relevant doses using cheaper & faster MS/MS methods " Safety up to therapeutic doses often preferable vs. microdoses " PD may save costs & time (if assessable within 14 days), e.g., receptor modulations with time (CNS) or steady-state PK " For biologics with short t 1/2 (often no appropriate animal model!)? " (Bayesian) PK, PK-PD modeling may be useful for predictions Drawbacks: " Time too short for biologics with long t 1/2, immunogenicity etc. " Do GMP requirements will still be a major hurdle for ECTs? " Healthy subjects directly followed by patients are not foreseen! Earlier start in man But: Avoid vulnerable populations or justify! Exploratory trials (+ exceptions ) allow more flexibility! The exploratory status and specific objectives should be clearly mentioned in the submission and in the protocol! Rules to be respected are the same as for any clinical trial EU Directive 2001/20/EC (04 Apr 2001): approval for clinical trials by the competent authority (CA) of each member state! Scientific advice on exploratory / traditional Phase I trials may be requested from CA (not only exceptional cases)! Minor (time) changes for traditional Phase I/II studies only 16
17 ! Informed consent of trial subjects: no change - The investigator should fully inform the subject AND: - The subject gives written signed and dated informed consent to: 1) The trial involves research with no clinical benefit 2) About aspects of the trial that are experimental 3) Any risks / inconveniences associated to the chosen approach! Site facilities & personnel: no change - FiH studies in appropriate clinical facilities / conducted by trained investigators with necessary expertise for early-phase trials - Trained medical staff with previous experience for FiH studies - Understanding of the IMP, its target and mechanism of action! Dose escalation scheme: no principal change EXCEPT for limitations in maximum and duration of dosing in ECTs! Information from preceding dose(s): no change Consider: exposure / effect / safety from preceding dose(s)! The no. of subjects per dose increment depends on the variability of PK / PD parameters and trial objectives: No principal change! Stopping rules required: no principal change - An ECT should be stopped as soon the objective is reached OR when it appears that it will be impossible to reach it! Define processes & responsibilities for dosing of subjects, dose escalation and stopping the trial: no change 17
18 ! Candidate selection by microdosing (as possible before)! Chances of faster ICH-based Go/No Go decisions in humans Less pre-clinical requirements, BUT (pre-) clinical rework foreseeable! Some improvement of the ICH process of harmonization E.g. for pre-clinics and ECTs, pediatrics and women in clinical trials! Focus on PD, e.g., receptor occupancy & PK-PD According to the CPMP Position paper & FDA critical path initiative! Implementation of many guidance: new is MD microdosing! ECTs offer more flexibility, useful for a part of drug candidates For many drug candidates usual FiH studies might still be preferable! Previous experience point to still existing hurdles to use ECTs E.g., re-work, lack of biomarkers, GMP requirements 18