Diagnosis and Current Standard Treatments for Multiple Myeloma. Natalie S. Callander, M.D Professor of Medicine
|
|
|
- Lily McBride
- 5 years ago
- Views:
Transcription


1 Diagnosis and Current Standard Treatments for Multiple Myeloma Natalie S. Callander, M.D Professor of Medicine
2 Goals Introduce and/or compliment understanding of plasma cell disorders-mgus, SMM and symptomatic MM Explain common blood and urine tests- more with Dr. Wassenaar Explain importance of cytogenetics and FISH testing-prognosis Current FDA approved treatments for newly diagnosed disease Autologous stem cell transplantation- more with Dr. Dhakal



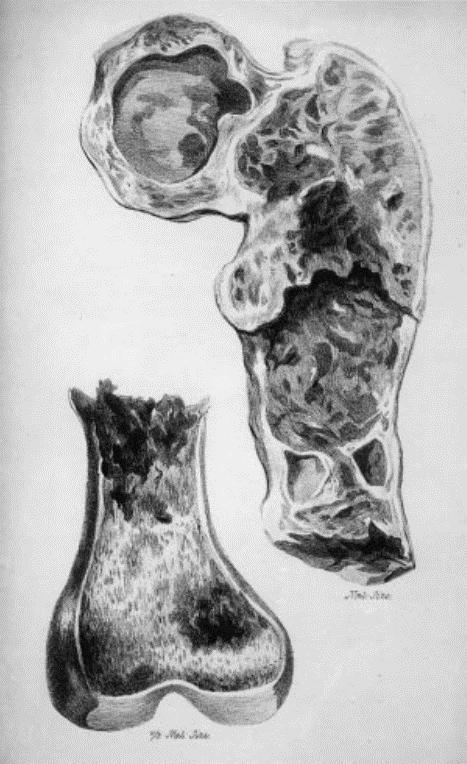

3 How long has myeloma been around?


4 Seer Data; Blood 125:410, 2015
5 Risk Factors Associated with Agent Orange exposure, benzene, radiation exposure (Hiroshima experience), 9/11 FR Higher incidence in farmers, wood and leather manufacturers Small Inherited Risk Landgren et al First degree relatives of 4488 Swedish MGUS pts had 3 X increased relative risk of Myeloma, WM, CLL, MGUS (Int J Cancer. 2006;118: ) Familial cases exist, 1q and 4q loci regions of interest for germinal genetic mutations; paratarg 7 (Grass et al Blood 2011:118:635) Not clear that there are specific polymorphisms, mutations that put pts at risk for development of myeloma
6

7 Normal B cell Development Normally, plasma cells are not found in large numbers inside bone marrow

8
9 Normal vs Myeloma IgG κ IgG L IgA κ IgA L IgD κ IgD L IgE κ IgE L IgM κ IgM L Normal Lots of different types of whole antibodies IgG κ IgG L IgA κ IgA L IgD κ IgD L IgE κ IgE L IgM κ IgM L IgG κ Myeloma 20 th Annual Update in Primary Care Whole Ab and excess light chains and too many of both! IgG κ





10 Symptoms:




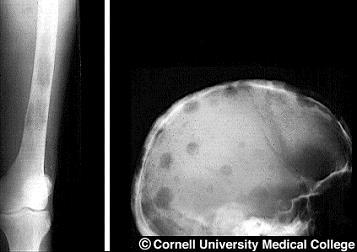
11 LYTIC BONE LESIONS lytic lesions like these can fracture.


12 Myeloma deposits can exist outside of bone marrow as well (just like lymphoma): require biopsy to prove plasma cell origin Extramedullary deposits

13 MRI offers ability to see inside of bones, standard of care to evaluate for spinal cord compression


14 PET-newer imaging tool for myeloma typically using fluorinated glucose to measure metabolic activity About 90% of myeloma pts show uptakei.e. some will not have informative PET Helpful for pts whose myeloma does not make protein May help predict response Likely will become part of initial evaluation

15
16 Laboratory testing: Interpretation of SPEP (serum protein electrophoresis)
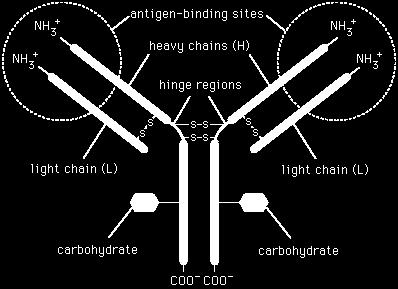
17 Immunoglobulin molecule
 and light chain (kappa or lambda)of the monoclonal")
18 Immunofixation of serum or urine (abs IFE) Identifies type of heavy chain (G, A, rarely D) and light chain (kappa or lambda)of the monoclonal protein


19 ex Excess protein in urine Makes suds
20 UPEP- sensitivity to pick up abnormal proteins varies from lab to lab NORMAL

21 Free Light Chain Assay: measures levels of kappa, lambda NOT bound to heavy chains
22 Free light assay- designed to detect portions of unbound light chains in serum Automated Results reported out in mg/l of mg/dl and in κ/λ ratio At low concentrations, lower specificity and sensitivity, or if pt has kidney failure significant values > 100mg/L or 10 mg/dl or abnormal ratio (<.015 or >8) Levels>100mg/dl now definition of myeloma Also ay be used for following amyloidosis pts or confirming CR, or possibly non secretory MM REMEMBER: normal value of M protein is 0; but it is normal to have light chains at low levels

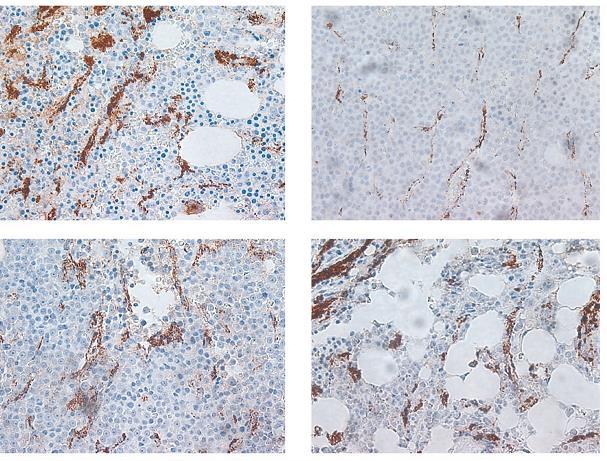
23 In order to definitively diagnose myeloma, a biopsy must show increase in plasma cells > 10%

24 Pathologist must prove clonality by IHC staining Plasma cells can be identified as well by CD 138 expression on flow cytometry
 are important")
25 Cytogenetic and Fluorescence In Situ Hybridization (FISH) are important prognostic tools
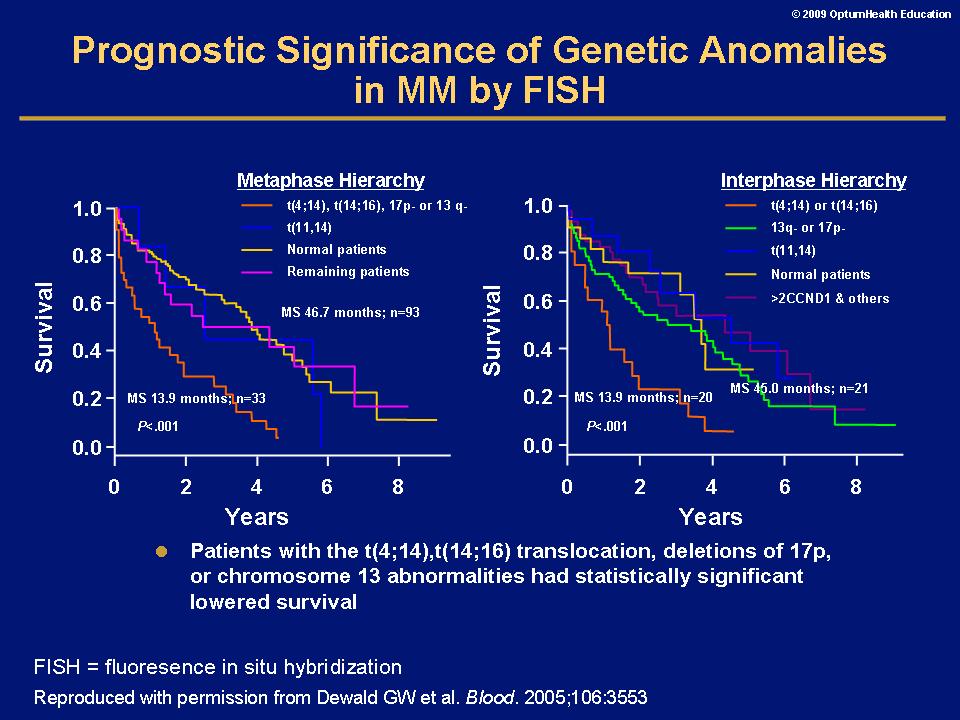
26
27 27
28 Finding small amounts of myeloma cells in bone marrow after treatment may have some importance

29
30

31 What happens to people with MGUS
32 Among adults age 50 3% have MGUS, 10% of 80 year old The prevalence of MGUS therefore makes SPEP/UPEP/light chains poor screening tests 75% of pts with MGUS will never develop myeloma Times to consider adding these tests to an evaluation-unexplained renal failure, proteinuria, osteoporosis in a young person, anemia

33
34 SMOLDERING MYELOMA DEFINITIONS DIFFER INTERNATIONAL CONCENSUS CRITERIA: M protein > 3 g/dl >10% but <60% plasma cells in marrow no end organ damage Some use a flow cytometry definition no renal insufficiency, bone damage (including osteopenia or any lesion found by MRI), anemia, hypercalcemia, recurrent bacterial infections
35 these patients progress much more often to myeloma- RISK OF PROGRESSION 10%/year risk factors for progression include: IgA vs IgG, low uninvolved immunoglobulins, sheets of plasma cells on bone marrow biopsy, presence of urinary light chains after five years, risk reverts to MGUS risk Clinical trials underway to see if early intervention will prevent most patients from progressing to myeloma
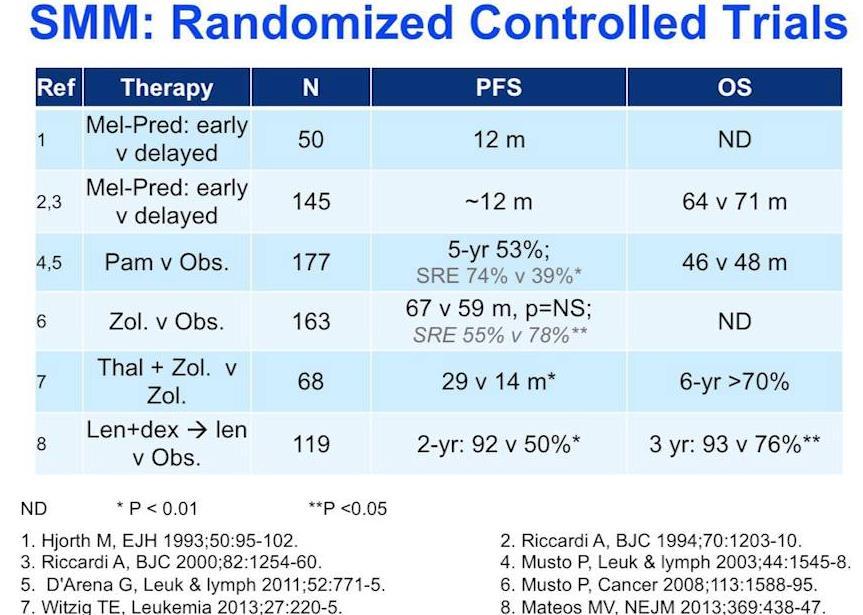
36



37 Plasmacytoma-isolated collection of myeloma cells Isolated plasmacytomas- about 5% Soft tissue based-sometimes isolated; often cured with radiation therapy Bone based-typically progress to myeloma in several years
38 Solitary Plasmacytoma
39 Solitary plasmacytoma (cont)
40 Long term prognosis

41
42
43 When should you start treatment for myeloma? Unlike lymphomas, stage of myeloma doesn t tell you what treatment is appropriate or when it should start MGUS should not be treated outside of clinical trial Symptomatic from myeloma Asymptomatic but with CRAB/IWMG criteria Smoldering or otherwise asymptomatic can wait with reasonably close follow up Patients with renal failure due to myeloma should be treated promptly

44

45 What are the clinical trial phases? Phase I Phase II Phase III Tests Safety Tests how well treatment works Compares new treatment to standard treatment


46 Limited treatment for myeloma In the first half of 20 th centuryradiation, pain medication
47
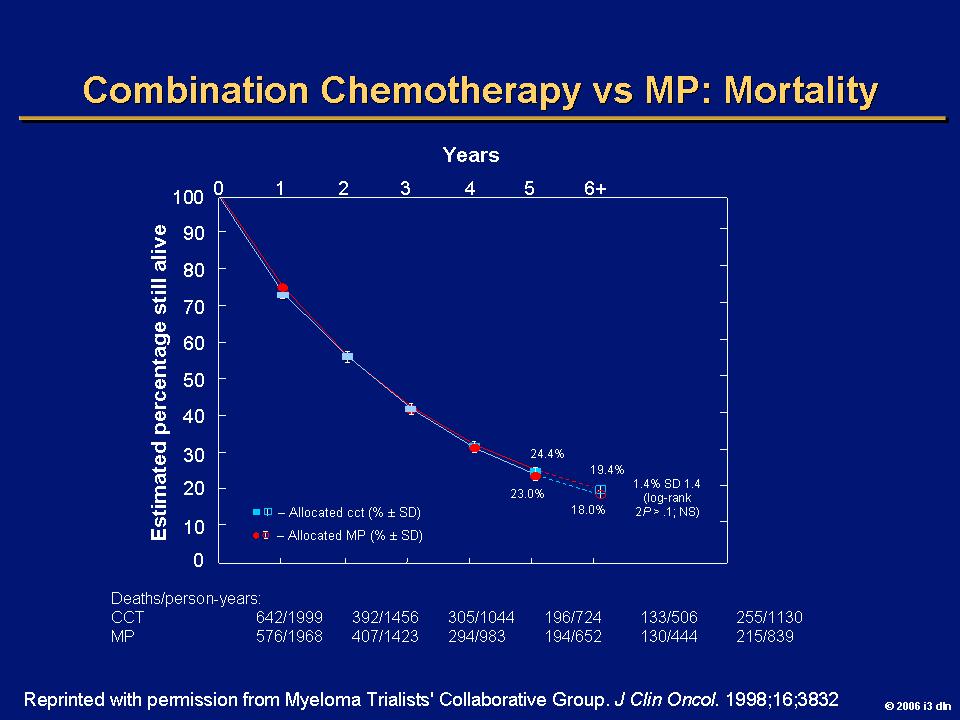
48

49 Traditional cancer drugs only work for the short time a cell actively replicating DNA in order to divide Myeloma cells grow slowly and don t spend much time doing this



50 Modern Age of Myeloma Therapy: discovery of thalidomide for myeloma Sold between to treat morning sickness Banned in 1962 in US due to phocomelia Interest revived in drug after it was reported to be helpful in leprosy in 1965 Suggested as useful in myeloma due to antiangiogenic properties
51 Kaplan Meier Estimates of Overall Survival and Event-free Survival. Singhal S et al. N Engl J Med 1999;341:
52
53 Thalidomide/Dexamethasone vs Dexamethasone in Newly Diagnosed MM Phase III ECOG E1A00 Study Design Newly diagnosed, untreated symptomatic MM (n=207) Thalidomide, 200 mg/d orally Dexamethasone, 40 mg/d* Days 1 4, 9 12, and (n=103) 4 cycles Dexamethasone alone, 40 mg/d* Days 1 4, 9 12, and (n=104) CR/PR/ stable Any progression Stop therapy at Month 4 for stem cell transplantation or continue at physician s discretion Stop therapy *Administered as a monthly cycle All patients received monthly pamidronate or zoledronic acid Rajkumar SV et al. Blood. 2004;104(part 1):63a [abstract 205]

54 NF-kB inhibition by Velcade (Bortezomib)
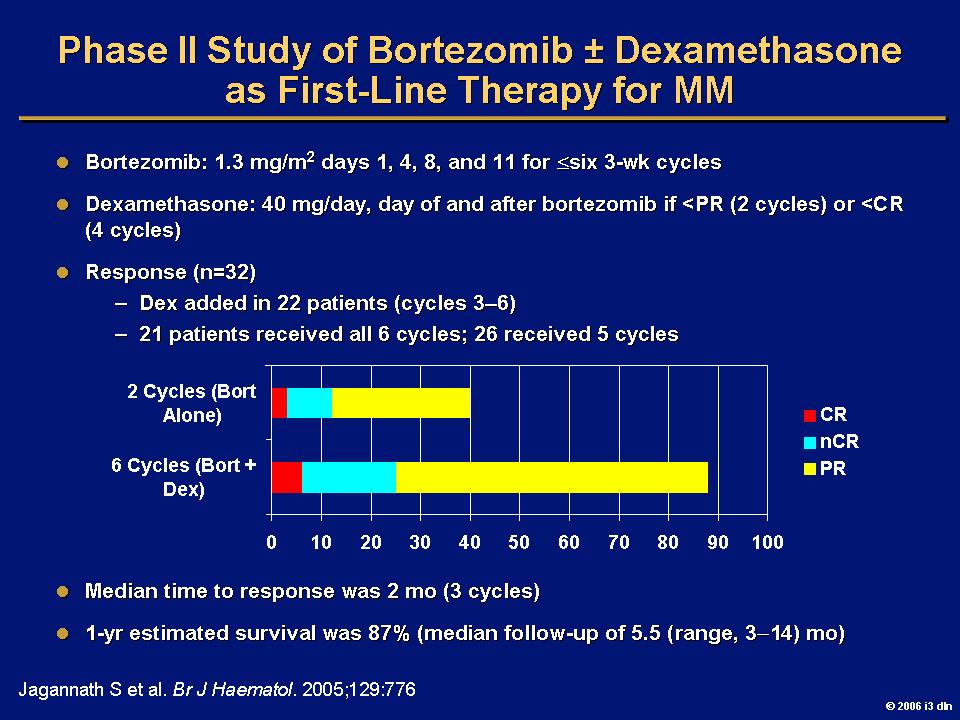
55
56
57

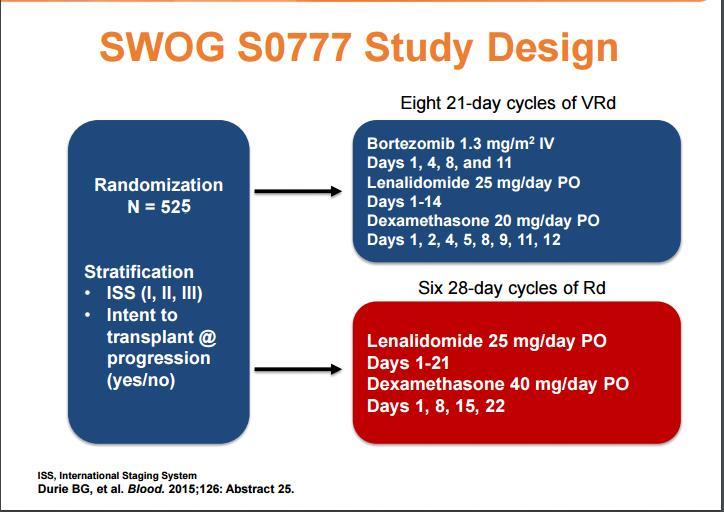
58 VRD is the current Standard of Care Multivariate analysis showed that receiving VRD, age <65 associated with Better disease control and survival
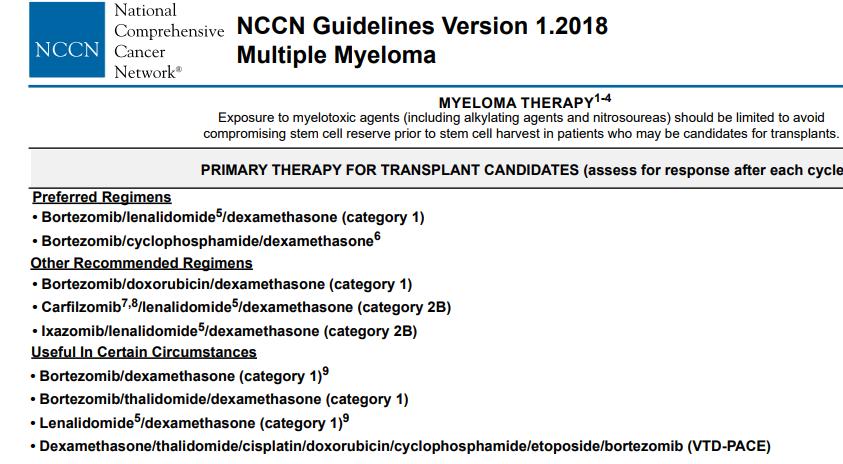
59 How else do you decide appropriate initial treatment? 1. Availability of clinical trials 2. Host characteristics (age, Performance Status, comorbidities) 3. Disease aggressiveness-high risk versus standard risk cytogenetic 4. Intent to transplant
60

61
62 High Risk Disease (75% of pts have what is termed standard risk myeloma (hyperdiploidy, t(11;14), t(6:14) MS->8 yrs 15% have high risk (17p, t(14;16), t(14;20) high risk GEP MS-2-3 yrs; high LDH, plasma cell leukemia triplet therapy (VRD, carfilzomib RD, VDT, CVRD, possibly VRD plus additional agent Extended or indefinite maintenance Or Auto stem cell transplant or allogeneic stem cell transplant followed by maintenance CLINICAL TRIAL RESULTS PENDING: SWOG S1211: VRD versus VRD plus elotuzumab
63 Other combinations under study for newly diagnosed pts S0777 has confirmed value of triplet therapy Not yet considered STANDARD outside of trial Carfilzomib, lenalidomide, dex Daratumumab, lenalidomide, dex Daratumumab, bortezomib, dex Daratumumab, lenalidomide, bortezomib, dex Elotuzumab, lenalidomide, dexamethasone Carfilzomib, daratumumab, lenalidomide, dex
64 Special considerations: Some patients may be too frail for intensive therapy, frequent clinic or hospital visits. First trial: continuous lenalidomide and dex based on results of FIRST trial; low dose VRD or CyBorD possible as well
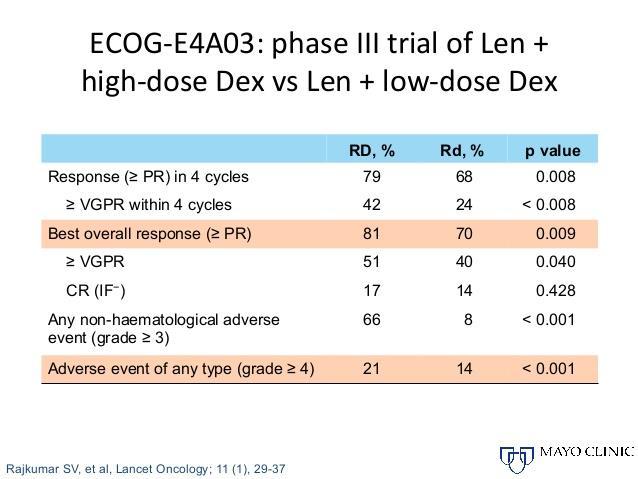
65 Lenalidomide and Dex may be very appropriate for some patients

66 High Dose Therapy for Myeloma Lancet 322: 822, 1983
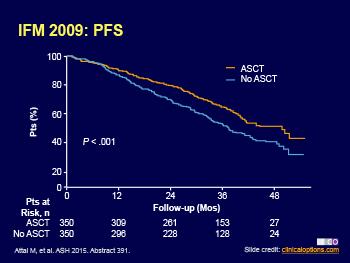
67 Autologous transplant improves disease control and survival Attal M et al. NEJM N Engl J Med 1996; 335:91-97

68
69
70
71
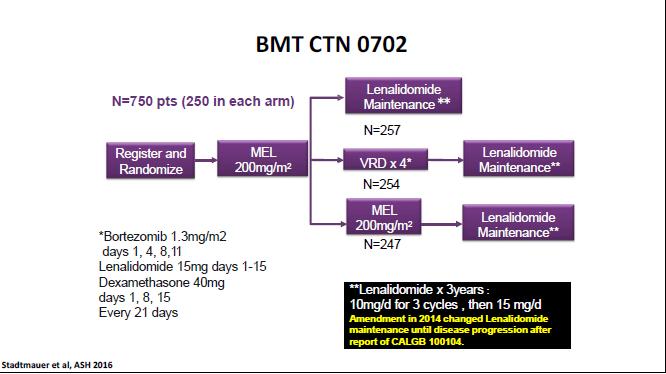
72 Maintenance Therapy CALGB : Post transplant, Randomization to Lenalidomide or Placebo Treatment given indefinitely Holstein S et al In press
73 Lenalidomide Maintenance After ASCT in MM: Meta-analysis Studies 3 of 17 identified studies fulfilled criteria [1] Study Treatment Arms Pts, n CALGB [2] IFM [3] GIMEMA [4] (RV-MM-PI-209) Lenalidomide maintenance Placebo Lenalidomide maintenance Placebo Lenalidomide maintenance No maintenance Lenalidomide maintenance intended to be given until progression IFM elected to discontinue lenalidomide in 2010 due to second primary malignancy signal, whereas the NCI and GIMEMA chose to continue until progression 1. Attal M, et al. ASCO Abstract McCarthy PL, et al. N Engl J Med. 2012;366: Attal M, et al. N Engl J Med. 2012;366: Palumbo A, et al. N Engl J Med. 2014;371: Slide credit: clinicaloptions.com 67 68
74 Lenalidomide Maintenance After ASCT in MM: Pooled Patient Characteristics Characteristic Lenalidomide (n = 605) Control (n = 604) Median age, yrs yrs of age or older, % ISS stage at diagnosis, % I II III CR/VGPR after ASCT, % Prior lenalidomide induction, % Adverse risk cytogenetics,* % *t(4;14) or del(17p); from IFM and GIMEMA studies only Attal M, et al. ASCO Abstract Slide credit: clinicaloptions.com
75 Lenalidomide Maintenance After ASCT in MM: Overall Survival Lenalidomide maintenance significantly improved survival after ASCT from pooled data analysis 7-yr OS: 62% vs 50% in the control arm Median OS: not estimable* vs 86.0 mos in control arm (median follow-up: 80 mos) Overall HR: 0.74 (95% CI: ; P =.001) All studies showed lenalidomide benefit, but results were heterogeneous (P =.047) CALGB HR: 0.56 (95% CI: ) IFM HR: 0.91 (95% CI: ) GIMEMA HR: 0.66 (95% CI: ) *Median OS for lenalidomide arm extrapolated to be 116 mos based on median of control arm and HR of Attal M, et al. ASCO Abstract Slide credit: clinicaloptions.com
76

77

78
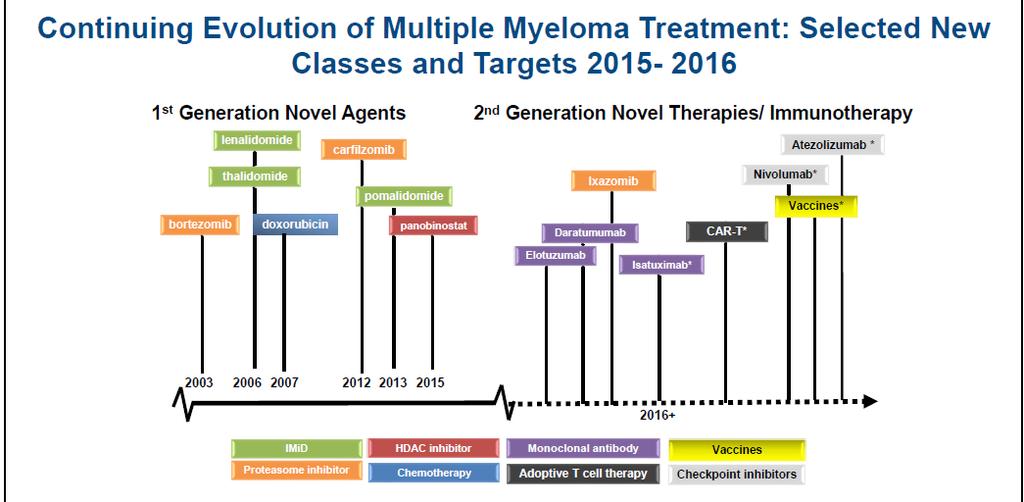
79 Summary of frontline therapy. Philippe Moreau et al. Blood 2015;125: by American Society of Hematology Dr. Hari will discuss Treatments for relapsed disease

80 SURVIVAL HAS NEVERY BEEN LONGER Kenneth C. Anderson Clin Cancer Res 2016;22: by American Association for Cancer Research

81
82 Bisphosphonates Developed in mid 1990s for bone strengthening properties and treatment of hypercalcemia (Berenson, NEJM) randomized trial of pamidronate vs. placebo in patients with MM for 2 yrs.->40% reduction in skeletal events, pain Zoledronate, pamidronate used more than alendronate Higher bioavailability Less GI toxicity

83 Same pt after rx, transplant, Bisphosphonates, 18 mo later KEY TO BONE HEALTH: CONTROL MYELOMA!

84 Study Design Presented By Noopur Raje at 2017 ASCO Annual Meeting
 Presented By Noopur Raje at 2017 ASCO Annual")
85 Results: Exploratory Endpoint Only small phase 2 studies of denosumab in relapsed myeloma; no effect on disease progression (Vij et al Am J Hematol :650) Presented By Noopur Raje at 2017 ASCO Annual Meeting


86 Exercise May reduce inflammation Helps pain, depression


87
88 CLINICAL TRIALS UNDERWAY NOW: THESE ARE THE KEY TO IMPROVING SURVIVAL S1211- high risk MM pts will do better with four drugs (including an antibody drug) rather than the three best drugs E1A11-is carfilzomib better than bortezomib? Length of maintenance CTN1401- making a personalized vaccine to give to a MM pt after a transplant will help them repel myeloma, much like a vaccine does for shingles, etc.
89
90 Conclusions Myeloma is a devastating disease However, MM patients living longer than ever before; this is due largely to clinical trials and new drugs that have incrementally improved survival Increasing number of choices for initial treatment COST WILL BE HUGE ISSUE NOW AND IN THE FUTURE CLINICAL TRIALS CAN SHOW US THE WAY!!!!