B cells Harry W Schroeder Jr MD PhD
|
|
|
- Sharon Spencer
- 5 years ago
- Views:
Transcription
1 B cells Harry W Schroeder Jr MD PhD Division of Clinical Immunology and Rheumatology Departments of Medicine, Microbiology, and Genetics University of Alabama at Birmingham Director, UAB Program in Immunology
2 Disclosure Nothing to disclose
3 Learning Objectives Upon completion of this session, participants should be able to: Review how B cells develop Review the clinical consequences of disruptions in B cell development or function
4 Genesis B cells - progeny of hematopoietic stem cells Development 7-8 wks gestation, pre-b cells appear in fetal liver wks gestation, pre-b cells appear in fetal bone marrow After birth, pre-b cells limited to bone marrow
5 Summary Antibody insufficiency can best be interpreted by taking into account where B cell development has failed: 1. Inability to produce immunoglobulin 2. Inability to produce a B cell receptor complex 3. Inability to signal properly through the BCR 4. Failure to receive T cell signals 5. Failure to modify immunoglobulin genes 6. Failure to receive or act on survival signals
6 Genesis Developing B cells use gene rearrangement to construct their antigen receptor Immunoglobulin rearrangement is hierarchical H chains first L chains second, before B cells must pass developmental checkpoints First test immunoglobulin integrity Then test binding specificity
7 Early Stages of B cell Development Immunoglobulin rearrangement Initial testing of the receptor Positive selection H chain must form a stable, signaling receptor with surrogate, and then conventional, light chain Signals through the BCR are required, suggesting a low level of self-reactivity is beneficial Negative Selection unacceptable self-reactivity Anergy Elimination Apoptosis, or Rescue by Receptor Editing
8 B cells in the Bone Marrow
9 Early Checkpoints
10 Signal transduction in B cells Two "domains" in the BCR complex Membrane Ig (mig or the BCR) Ig /Ig CD79 BCR binds antigen Ig and Ig transduce the signal Cytoplasmic tails contain immunoreceptor tyrosine-based activation motif (ITAM) Activate tyrosine kinases (Src family)
11 Alternative Splicing Yields Secretory or Membrane Ig (BCR) CH L V DJ J S M1 M2 Alternative Splicing CH L V DJ J S M1 M2 CH L V DJ J S M1 M2 AAA AAA V DJ C M V DJ C S B cell Receptor Ig Ig Soluble Immunoglobulin
12 Key Concepts Primary B cell Development B cell development can be viewed as a linear, step-wise process focused on the assembly and testing of immunoglobulin function, first in the fetal liver and bone marrow, and then in the periphery Expression of a functional receptor subjects the B cell to antigen selection B cells with inappropriate specificities tend to be eliminated or inactivated by apoptosis, receptor editing, or anergy
13 B cell Development (Human) Vale and Schroeder, JACI in press, 2010
14 Clinical Consequences B cells will not be made in normal numbers if there is: Failure to create immunoglobulin e.g. RAG deficiency, C deletion Failure to create the BCR e.g. 5/14.1, VpreB, Ig (CD79a), Ig (CD79b) deficiency Inability to properly signal through the BCR e.g. BLNK (AR), BTK deficiency(xl)
15 Clinical Consequences Failure to properly limit RAG mediated rearrangement to VDJ joining can create dangerous mutations e.g. transfer of an IgH promoter or enhancer activates anoncogene Burkitt s Lymphoma (IgH c-myc) Follicular Lymphoma (IgH Bcl2)
16 Key Concepts Primary B cell Development B cell development can be monitored by examining the pattern of expression of lymphoid-specific surface proteins Antibodies against these surface proteins can be used to eliminate B cells e.g. Rituximab (anti-cd20)
17 B cell Development (Human) Vale and Schroeder, JACI, 2010
18 Transition Bone Marrow CD19 + cells If the immature IgM-only B cell is highly self-reactive, it can be eliminated by receptor editing or apoptosis, or neutralized by anergy As the B cell matures, it begins to express IgD in addition to IgM Mature B cells that express IgD as well as IgM are programmed to respond to antigen, rather than be eliminated by antigen
19 Clinical Consequences Failure to prevent the formation of antibodies with high avidity or high affinity to self-antigens can lead to autoimmunity e.g. Myasthenia gravis, SLE
20 IgM and IgD via Differential Splicing CH L V DJ J S M1 M2 CH S M1 M2 Alternative Splicing L V DJ J S M1 M2 CH CH S M1 M2 AAA V DJ C M migd Ig Ig
21 Survival in the Periphery Until the B cell makes a contact with an antigen it can recognize, it must survive in the primary follicle Follicles contain dendritic cells that release "survival" signals, such as BLyS (BAFF) There is presumed to be competition between newly formed B cells and naïve B cells for space in the follicle The mature B cell has a limited time to find its antigen before it dies

22 BLyS Family Ligands and Receptors Modified from Crowley et al, Semin Immunol 17, 193 (2005)
23 Modulation of B cell signals Activation CD19, CD21, & TAPA-1 Complex CD19, a member of Ig superfamily CD21 (CR2), a receptor for C3d CD81 (TAPA-1), a transmembrane protein ITAM Motifs Inhibition CD22 Fc RII ITIM Motifs
24 Initial Activation Ag Ag CD21 CD19 CD81 ITAM ITAM Activation
25 Upregulation of B cell signals C3d Ag Ag CD21 CD19 CD81 ITAM ITAM Activation
26 Downregulation of B cell signals Fc RII C3d Ag Ag CD21 CD19 CD81 ITIM ITAM ITAM Inhibition Activation
27 Clinical Consequences Abnormal antibody responses in the presence of B cells (CVID, IgAD) Alteration of BCR signals CD19 deficiency (AR) Defective B cell survival signals TACI, BAFFR alterations or deficiency (AR, AD)
28 Three Types of Mature B cells B-1 cells Self-renewing and preferentially produced in the fetus Spontaneously produce polyreactive Igs In mouse: CD5 +, Mac-1 + *In human: CD20 + CD27 + CD43 + CD70 -
29 Three Types of Mature B cells Marginal Zone B cells Found in the marginal zone of the spleen May also be found in the blood Pre-activated Respond quickly to antigens, e.g. polysaccharides
30 Three Types of Mature B cells B-2 cells ( Conventional B cells) Preferentially produced after birth Replaced in bone marrow Typically respond to protein Ag, requiring T cell help

31 Three Types of Mature B cells
32 Late Stages of B cell Development Exposure to antigen in the periphery Activation Class switching and somatic hypermutation Selection for receptor specificity and affinity Differentiation into plasma or memory B cells
")
33 T-Independent Responses Type 1 Mitogens (LPS) Type 2 Polymeric (polysaccharides, bacterial flagellin)

34 Rapid Activation of Marginal Zone B cells in Response to Strep. pneumoniae Lopes-Carvalho and Kearney, Immunol Rev 197:192 (2004)
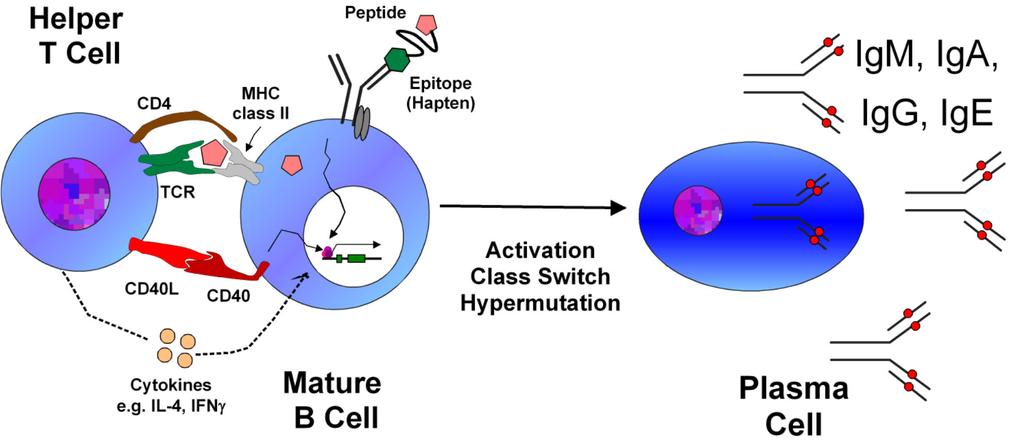
35 T-Dependent Responses
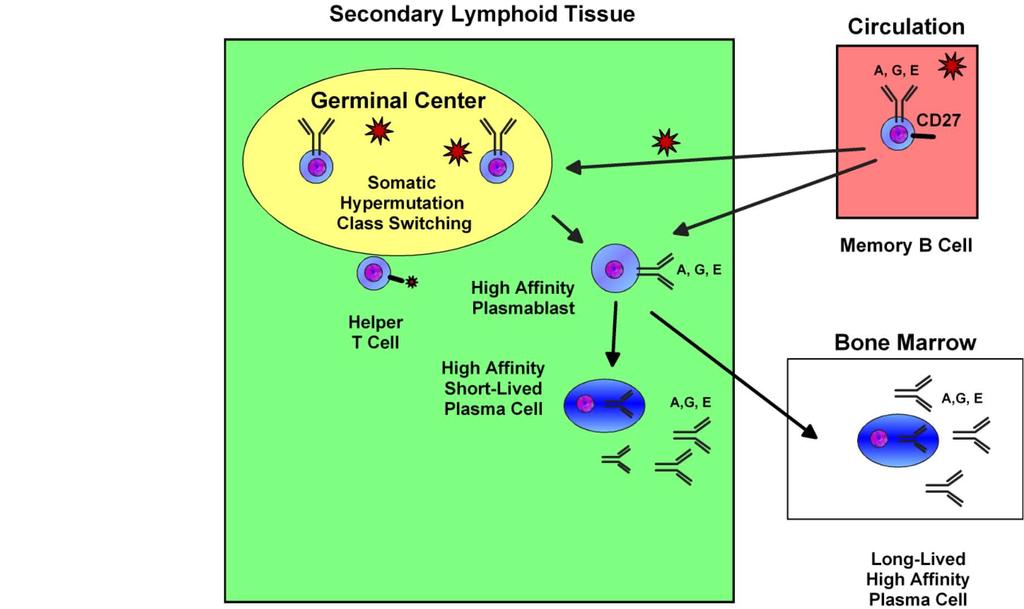
36 Somatic Hypermutation and Affinity Maturation Occurs in response to antigen Primarily occurs in the dark zone of the germinal center Typically requires T cell help Mutated antibodies subjected to competition Increased affinity = Success Affinity Maturation
37 Deamination C U
38 AID and Somatic Hypermutation
39 Somatic Hypermutation Primary Day 7 Day 14 H chain V Domain L chain V Domain Relative Affinity Class CDR1 CDR2 CDR3 CDR1 CDR2 CDR3 V D J V J +/- +/- +/- + +/ / /- Secondary Replacement Silent

40 Encounter with an Antigen

41 Meet a Friendly Follicular Helper T cell
42 Live Life in a Burst of Glory or Grow
43 Antigen-Driven Differentiation
44 Antigen-Driven Differentiation
45 Class Switching Occurs by gene rearrangement Mediated by AID instead of RAG Involves non-homologous recombination between a pair of switch sites rather than pairs of RSS The switch sites are composed of multiple G/C rich nucleotide repeats Transcription of the switch site is required Initiation of transcription is driven by T cell cytokines (e.g., IL-4 drives IgE and IgG4 in human) L V DJ C C C C C C C C C 5' 3' S S S S S S S S
46 AID and Class Switching
47 Recombination Occurs by Deletion Initial recombination occurs between S and a downstream S site AID induces double strand breaks in both S regions, which when spliced together, delete the intervening sequence Allows switching from IgM to IgG, IgA or IgE IgD is an exception (no switch region) L V DJ C C C C C C C C C 5' 3' S S S S S S S S Sequential Class Switch L V DJ C C 5' 3' S S L V DJ C 5' 3' S
48 Key Concepts Peripheral B cell Development T-independent activation of naive B cells causes them to develop into either short-lived plasma cells or long-lived B1 cells. T-dependent activation of B cells leads to germinal center formation, permitting somatic hypermutation and class switch recombination.
49 Key Concepts Peripheral B cell Development T-dependent activation of naive B cells results in differentiation into either memory B cells or short-lived plasma cells. T-dependent activation of memory B cells either results in expansion of memory B cells or differentiation into long-lived plasma cells.
50 Clinical Consequences Abnormal antibody responses in the presence of B cells (Hyper IgM Syndrome) Failure of helper (follicular) T cell B cell interactions e.g. X-linked CD40 ligand deficiency, CD40 deficiency Failure to modify immunoglobulin genes (SHM and/or CSR) e.g. AID deficiency, UNG deficiency
51 Clinical Consequences Failure to limit the action of AID to the Ig V domains can create dangerous mutations e.g. Aberrant mutations have been found in both regulatory and signaling genes from normal human B cells and B lymphomas. This includes Bcl6, CD95 and c-myc
52 Two Types of B cell Memory


53 Three Types of Memory B cells
54 Ontogeny of Immunity 70 pre-b B 19 Average CDR-H3 Length (in codons) % of Lymphoid Cells Birth Age (Weeks) 0 Fetus Age in Years Modified from: Schroeder HW, et al. Blood 98:2745 (2001) Modified from: Nunez C, et.al, J. Immunol. 156:866 (1996)
55 Clinical Consequences Antibody responses in infants differ from those of adults in terms of both quantity and quality
56 Summary Antibody insufficiency can best be interpreted by taking into account where B cell development has failed: 1. Inability to produce immunoglobulin 2. Inability to produce a B cell receptor complex 3. Inability to signal properly through the BCR 4. Failure to receive T cell signals 5. Failure to modify immunoglobulin genes 6. Failure to receive or act on survival signals