Fecal transplant: Con Position
|
|
|
- Eleanore Barnett
- 5 years ago
- Views:
Transcription
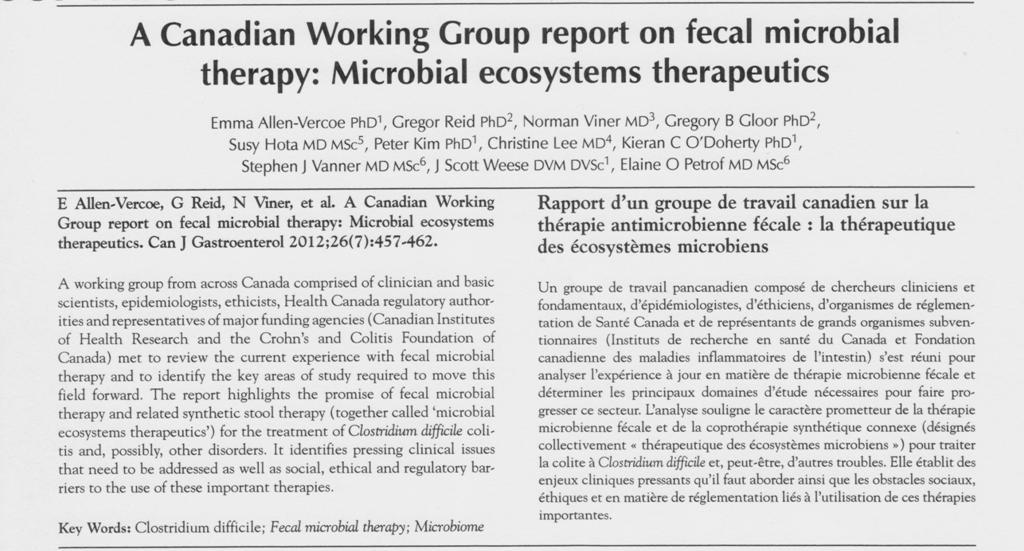
1 Fecal transplant: Con Position Elaine O. Petrof, MD, MSc Dept.Medicine Division of Infectious Diseases Gastrointestinal Diseases Research Unit Queen s University ISAPP Meeting Cork, Ireland Oct.1 st, 2012
2 What is the evidence? Recurrent C.difficile focus is on this area Meta-analysis of case series, case reports However randomized clinical trials comparing this treatment to standard of care have yet to be published.

3
4 Problems identified with fecal transplants lack of standardization risk of infection transmission from the donor psychological barriers (freshly defecated fecal matter) limitations in donor screening turnaround times standard laboratory screening - does not detect all pathogens slow mobilization / screening of donors can be a barrier to timely treatment when patients are acutely ill

5 Ref: Allen-Vercoe et al., Can J Gastroenterol., 26(7):457-62, 2012
6 Synthetic Stool to replace stool transplant: A possible alternative?
7 Synthetic Stool - Advantages 1. Exact composition of bacteria administered would be known and controlled 2. Mixture can be reproduced if future treatment necessary 3. More stable than stool, which [ideally] is collected fresh and used within 6 hours of collection 4. Absence of viruses and other pathogens in the administered mixture (patient safety) 5. Less unpleasant - psychological/ sociological stigma associated with using stool is eliminated

8 ROBOGUT - allows simultaneous support of 6 independent bacterial communities - capacity to examine microbial communities from 6 different human donors simultaneously

9 Healthy female Age 41 at time of collection Average BMI Very healthy lifestyle The donor 1 reported exposure to antibiotics in the last 10 years >70 strains isolated from fresh feces or Robogut culture 1 donor for 1 ecosystem: We hypothesize that the derived ecosystem, naturally selected in the donor, will be ecologically more stable than a similar derived ecosystem from many donors







10 RePoopulate (RP) 33 strains - selected for favourable antimicrobial susceptibility Identified by 16S rrna sequencing Cryopreserved at -80 C as individual strains Cultured as separate components on complex media Tested for ecosystem stability in the Robogut Ref: Petrof et al., Microbiome 2012, in press

11 RePoopulate (RP) MetaRep (datasets from Healthy Donors) used as a guide for relative species abundance for RP mixture (by biomass) estimated concentration of 3.5 x109 CFU/mL 100 ml pre-reduced sterile 0.9% normal saline used within 24 hours of preparation vancomycin held 48hrs prior to treatment administered by colonoscopy Ref: Petrof et al., Microbiome 2012, in press

12

13

14 Ref: Petrof et al., Microbiome 2012, in press
 No diarrhea, no abdo pain Shannon diversity")
15 Microbial diversity: not the whole story? Symptomatic (diarrhea, abdo pain) No diarrhea, no abdo pain Shannon diversity index values for the RP and patient samples
16 Microbiome comparison of the patient and RP samples: Changes in the composition of the human gut microbiome 4 weeks after RePOOPulate is a composite of RP and recipient microbiota
17
18 Summary It is possible to create a therapeutic ecosystem to treat C.difficile infections may be a feasible alternative to conventional stool transplants Probably more safe - certainly more broadly reproducible - than conventional FMT More research needed in this area Decreased diversity may be less important than the actual organisms in the mixture We hope to augment formulations with microbes that are antagonistic towards C.difficile

19 Acknowledgements Queen s University Curtis Noordhof (Petrof lab) Adriana Breen Dr.S.Vanner KGH Clinical Staff Funded by: University of Western Ontario Dr. Greg Gloor University of Guelph Dr.Emma Allen-Vercoe & lab Dr. Scott Weese