Multiple Myeloma and Related Disorders. Zsolt Nagy
|
|
|
- Marjory Campbell
- 5 years ago
- Views:
Transcription

1 Multiple Myeloma and Related Disorders Zsolt Nagy
2 Outline Biology Plasma Cell Dyscrasia MGUS Plasmacytoma Multiple myeloma Smoldering POEMS Waldenstrom s Macroglobulinemia Amyloidosis
3 Classification of Monoclonal Gammopathies Monoclonal Gammopathy of Undetermined Significance Malignant Monoclonal Gammopathies Multiple Myeloma Smolderimg Multiple Myeloma Plasma cell leukemia IgD myeloma POEMS Plasmacytoma Malignant Lymphoproliferative disorders Heavy Chain disease Amyloidosis

4

5 Normal B-cell Development Lymph Node IgM Lymphoplasmacyte (memory B Cell) ::... IgM Short-lived plasma cell Follicle center Lymphoblast Plasmablast Somatic Hypermutation of Ig Sequences Stimulation with Antigen Naïve B Cell Isotype Switching Bone Marrow ::... G, A, D, E Long-lived plasma cell Pre-B cell
6 B cell Development As a Framework for Malignancies Lymphoplasmacyte IgM Lymph node Germinal Center SOMATIC HYPERMUTATION Plasmablast Lymphoblast SWITCH RECOMBINATION Virgin B cell Bone Marrow G,A,E Plasma cell V(D)J RECOMBINATION Pre-B cell
7 B cell Development As a Framework for Malignancies Lymphoplasmacyte IgM WALDENSTROM S Lymph node Germinal Center SOMATIC HYPERMUTATION Plasmablast FOLLICULAR LYMPHOMA Lymphoblast BURKITT S LYMPHOMA Virgin B cell CLL Bone Marrow MULTIPLE MYELOMA G,A,E Plasma cell ALL Pre-B cell
8 The Continuum of Plasma Cell Disorders Normal MGUS Indolent Multiple Myeloma Myeloma
9 Myeloma, Malpas et al. 2004

10
11 The hallmark of plasma cell disorders is the presence of a paraprotein in the serum and/or urine.
12 Paraproteinemias Normal immunoglobulin pattern Polyclonal reflects progeny of different plasma cells Paraproteinemia Monoclonal immunoglobulin band in sera reflects synthesis from single plasma cell clone
13 M-Protein Tests Urine Dipstick not sensitive to Bence Jones proteins, need sulfosalicylic acid (SSA) Screening (SPEP/UPEP) Gamma-globulins Polyclonal gammopathy: liver disease, connective tissue disease, chronic infection, others Hypogammaglobulinemia: Immunodeficiency, nephrotic syndrome (amyloidosis), myeloma/cll Monoclonality Immunofixation with monospecific antibodies Immunoelectrophoresis Immunoassay for serum free light chains (Mayo Clinic)

14

15 SPEP Polyclonal Gammopathy Monoclonal Gammopathy
16 Normal Immunoelectrophoresis

17

18
19 Presentation of Plasma Cell Disorders Increased protein on a routine chemistry panel Anemia Bone pain Renal dysfunction Hypercalcemia
20 Pathophysiology: Monoclonal B- Cells/Plasma Cell Dyscrasia Marrow replacement Cytopenias Constitutional symptoms Decreased quantitative immunoglobulins Infections Lytic bone lesions Fractures Hypercalcemia Extramedullary involvement Plasmacytomas Organomegaly
21 Pathophysiology: Monoclonal Immunoglobulin Proteins Heavy chains or Light chains in serum, urine, kidney or other tissues Renal insufficiency Neurologic disease Hyperviscosity Cold Agglutinin disease AL Amyloidosis POEMS: Polyneuropathy, Organomegaly, Endocrine disturbances, M-protein, Skin changes

22 MGUS: Monoclonal Gammopathy of Undetermined Significance
23 MGUS Diagnosis Serum M-protein Usually IgG or IgA, usually <3 g/dl Stable over time Marrow plasma cells <10% No lytic bone lesions, unexplained anemia, hypercalcemia, or renal insufficiency Incidence 1-2% of adults Increases with age 6% aged y/o, 14% >90 y/o

24
25 Monoclonal Gammopathies Mayo clinic SMM 4% (39) LP 3% (37) AL 8% (90) Extramedullary 1% (8) Macro 3% (30) Other 3% (33) MGUS 62% (659) MM 16% (172)

26
27 MGUS Progression 1384 patients at Mayo MGUS: 1% per year progression Relative risk 25x (myeloma), 46x (Waldenstrom s), 8.4x (amyloid), 2.4x (lymphoma) IgM MGUS: 1.5% per year Predictors Size of M-spike (> 2.5 g/dl, 41% at 10 yr) Serum albumin NEJM 2002;346:564. Kyle ASH 2002 #384.

28

29 Risk of progression of MGUS to myeloma or related disorder using a risk-stratification model that incorporates the FLC ratio and the size and type of the serum monoclonal protein. Rajkumar S V et al. Blood 2005;106: by American Society of Hematology
30 MGUS: Management Testing CBC, calcium, creatinine, SPEP with immunofixation, quantitative immunoglobulins, 24-hour urine protein (with UPEP and immunofixation if positive) If M-protein 2-3 g/dl, add bone marrow and skeletal survey F/U SPEP/H&P repeated in 6 months, then annually
31 Multiple Myeloma and Related Disorders Definition: A group of diseases that involve malignant proliferation of Ig-secreting cells of B-cell lineage that are usually associated with paraproteinemia or paraproteinuria.
32 Multiple Myeloma US Incidence: 15,000 new cases/year 1% of malignancies US Prevalence: 65,000 cases/year Double incidence rate in African Americans Median age 65 3% <40 years old Unknown cause Radiation, benzene, solvents, pesticides, insecticides
33 Etiology Etiology is not known. Risk factors: Race, sex. Increased risk with ionizing radiation and exposure to pesticides like Dioxin. Recently viruses like HHV-8 and SV-40, have been linked to myeloma development.
34 MOLECULAR PATHOGENESIS OF MYELOMA Lancet 2004;363:875

35 Myeloma Cells and BM Microenvironment Bruno et al, The Lancet Oncology, July 2004,
36 MM: Clinical Features Disease of the elderly (7th decade) Bone pain most commonly vertebra and long bones lytic lesions fractures
37 Myeloma: Clinical Features Bone pain: often with loss of height Constitutional: weakness, fatigue, and weight loss Anemia Renal disease: renal tubular dysfunction Infections: neutropenia/hypogammaglobulinemia Hypercalcemia: myeloma cells secrete osteoclast-activating factors Hyperviscosity: 2% with myeloma; 50% with macroglobulinemia Neurologic dysfunction: spinal cord or nerve root compression
38 Major Symptoms at Diagnosis Bone pain: 58% Fatigue: 32% Weight loss: 24% Paresthesias: 5% 11% of patients are asymptomatic or have only mild symptoms at diagnosis Kyle RA, et al. Mayo Clin Proc. 2003;78:21-33.

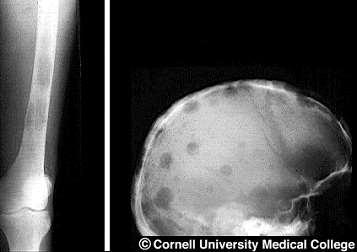
39 Multiple Myeloma Typical Punched Out Lesions

40

41

42

43 Multiple Myeloma
44 Diagnostic Criteria for Myeloma Patient Criteria MGUS [1,2] Smoldering Myeloma [1] M protein < 3 g/dl spike 3 g/dl spike and/or Monoclonal plasma cells in bone marrow, % End-organ damage *C: Calcium elevation (> 11.5 mg/l or ULN) R: Renal dysfunction (serum creatinine > 2 mg/dl) A: Anemia (Hb < 10 g/dl or 2 g < normal) B: Bone disease (lytic lesions or osteoporosis) Active Myeloma In serum and/or urine [2] < [2] None None 1 CRAB* feature [3] Only patients with symptomatic MM should be treated 1. IMWG. Br J Haematol. 2003;121: Kyle RA, et al. N Engl J Med. 2002;346: Durie BG, et al. Hematol J. 2003;4:

45
46 Myeloma Diagnostic Work-Up SPEP and UPEP (24 collection) with immunofixation 3% nonsecretory: check serum free light chains Skeletal survey (not a bone scan) Quantitative serum immunoglobulins (IgA, IgG, IgM) Bone Marrow Aspirate and Biopsy Other tests (calcium, creatinine, beta-2 microglobulin, CRP, albumin, plasma cell labeling index, etc, etc) are only for staging/prognosis
47 Myeloma Prognostic Work-Up Hemoglobin Calcium Serum creatinine Beta-2 microglobulin Albumin Bone Marrow cytogenetics FISH chromosome 13 and 11? C-reactive protein?? Plasma cell labeling index?? Serum IL-6??
48 Myeloma Renal Disease Myeloma kidney Normal glomerular function Concentrated light chains precipitate in tubules Monoclonal light chains seen in UPEP with immunofixation Glomerular lesions Deposits of amyloid or light chain deposition disease Nonselective leakage of all serum proteins UPEP preponderance of albumin



49 Renal Manifestations Myeloma Kidney Cast Formation Light chain Deposition Amyloidosis Pierre Ronco JNEPHROL 2000; 13 (suppl. 3):




50 Pathology
51 Myeloma: Durie-Salmon Staging Stage I Hemoglobin >10 g/dl Normal calcium No lytic bone lesions Low M-protein IgG <5 g/dl IgA <3 g/dl Bence Jones <4 g/24h Stage II (not Stage I/III) Stage III Hemoglobin <8.5 Calcium >12 (adjusted) >3 lytic bone lesions High M-protein IgG >7 g/dl IgA >5 g/dl Bence Jones >12 g/24h A) Creatinine <2 B) Creatinine >2
52 Myeloma: Median Survival Durie-Salmon stage Stage I Stage II Stage III 60 months 40 months 15 months

53 International Myeloma Working Group Revised Staging System
54 Therapy of Newly Diagnosed Multiple Myeloma: Kyle, Mayo Clin Proc, 2003.
55
56 Novel biologically based therapies targeting MM cells and the BM microenvironment Novel Agents Apoptosis Growth Arrest A B Inhibition of Adhesion Adhesion Molecule C Inhibition of Cytokines IL-6 IGF-1 VEGF SDF-1α Proliferation D bfgf VEGF Angiogenesis Drug Resistance
57 Novel Agents for Myeloma Targeting both MM cells and interaction of MM cells with the BM microenvironment Targeting circuits mediating MM cell growth and survival Targeting the BM microenvironment Targeting cell surface receptors
58 Novel Agents for Myeloma Targeting both MM cells and their interaction with BM microenvironment Thalidomide and its analogs (Revlimid) Proteasome inhibitor (Bortezomib) Arsenic trioxide 2-Methoxyestradiol (2-ME2) Lysophosphatidic acid acyltransferase-β inhibitor Triterpinoid 2-cyano-3, 12-dioxoolean-1, 9-dien- 28- oic acid (CDDO) N-N-Diethl-8, 8-dipropyl-2-azaspiro [4.5] decane-2-propanamine (Atiprimod) Targeting circuits mediating MM cell growth and survival VEGF receptor tyrosine kinase inhibitor (PTK787/ZK222584, GW654652) Farnesyltransferase inhibitor Histone deacetylase inhibitor (SAHA, LAQ824) Heat shock protein-90 inhibitor (Geldanamycin,17-AAG) Telomerase inhibitor (Telomestatin) bcl-2 antisense oligonucleotide (Genasense) Inosine monophophate dehydrogenase (VX-944) Rapamycin Targeting the bone marrow microenvironment Targeting cell surface receptors IĸB kinase (IKK) inhibitor (PS-1145) p38 MAPK inhibitor (VX-745, SCIO-469) TFG-β inhibitor (SD-208) TNF related apoptosis-inducing ligand (TRAIL) / Apo2 ligand IGF-1 receptor inhibitor ( ADW) HMG-CoA reductase inhibitor (statins) Anti-CD20 antibody (Rituximab)
59 Myeloma: Therapy Principles Observation for stage I Incurable despite conventional chemotherapy and high-dose therapy Bisphosphonates Chemotherapy Conventional High-dose with stem cell rescue New agents Graft-versus-myeloma
60 Myeloma: Supportive Therapy Bisphosphonates Phase III: monthly pamidronate (JCO 1998;16:593) Skeletal-related events 38% versus 51%, p=0.015 Median survival 21 versus 14 months Compression fractures: vertebroplasty DVT risk: steroids, steroids + thalidomide Hypercalcemia Renal insufficiency:?plasmapheresis Infections Anemia: Eyrthropoietins
61 Myeloma Bone Marrow Interactions Microenvironment Myeloma cell adhesion molecules react with stroma Release of osteoclast activating factors (IL-1B, IL-6, TNFB) Vascular endothelial growth factor (VEGF) secreted by myeloma cells Myeloma Bone Disease
62


63 Plasmacytoma
64 Extramedullary Plasmacytoma ~3% of plasma cell neoplasms Isolated plasma cell tumors of soft tissues Upper respiratory tract common Uninvolved marrow, negative skeletal survey M-protein present ~25% cases Disappears following treatment Curable with local radiation therapy
65 Solitary Plasmacytoma of Bone ~3% of plasma cell neoplasms One isolated bony lesion of plasma cells Uninvolved marrow <5% plasma cells M-protein present ~25% cases Disappears following treatment Curable with local radiation therapy Median OS 10 years Multiple myeloma develops in 50-60%
66 Osteosclerotic Myeloma (POEMS) Polyneuropathy Sensorimotor peripheral neuropathy in 75% Organomegaly Lymphadenopathy, hepatomegaly, splenomegaly Endocrinopathy Adrenal, thyroid, pituitary, gonadal, parathyroid, pancreatic M-Protein Skin changes Hyperpigmentation, hypertrichosis, plethora, hemangiomata, white nails


67 Ghobrial et al, Lancet Oncol 2004, Treon et al, Blood 2009
68 Lymphoplasmacytic Lymphoma (Waldenstrom s Macroglobulinemia) Malignant proliferation of plasmacytoid lymphocytes secreting IgM M-protein 1400 cases/year Organomegaly/Peripheral neuropathies Cryoglobulinemia Type I: Raynaud s phenomenon, cold urticaria, etc. Type II: Purpura, arthralgias, renal failure, mononeuritis IgM tissue infiltration/al amyloidosis Coagulation abnormalities

69
70 Consensus recommendations of the 4th International WM meeting First Line therapy: Combination therapy (RCD or CPR; Cytoxan+nucleoside analogues+r; R-CHOP, R-CVP) Rituximab single agent Nucleoside analogues Alkylators Salvage therapy: Re-use therapies Bortezomib Thalidomide+steroids Alemtuzumab AHSCT Dimopoulos, JCO 2009, Treon et al Clin Lymph and Myeloma 2009
71 Hyperviscosity Usually IgM >5 g/dl, viscosity >4.0 Eyes Sausage link conjunctival and retinal veins Retinal hemorrhages, Papilledema CNS Ataxia, nystagmus, vertigo, confusion, altered consciousness Increased intravascular volume Dilutional anemia Risk congestive heart failure with transfusion Therapy: plasmapheresis/chemotherapy
72 Waldenstrom s Macroglobulinemia: Therapy Plasmapheresis for hyperviscosity 2-Chlorodeoxyadenosine (2-CdA, cladribine) Fludarabine Rituximab Other myeloma-like therapies
73 Amyloidosis Extracellular tissue deposition of low molecular weight fibrils Beta-pleated sheets, bind Congo red Precursor proteins involved Monoclonal immunoglobulin light chains: Primary (AL) Amyloidosis Serum amyloid A protein: Reactive or Secondary (AA) Amyloidosis Beta-2 microglobulin: Dialysis (DA) Amyloidosis Transthyretin, apolipoprotein A-I, Alzheimer amyloid precursor protein, prion protein, Prolactin, Atrial natriuretic protein, Procalcitonin, Insulin, Keratin

74 Amyloidosis: Protein Misfolding Diseases ~30 proteins localized Amyloidosis systemic Amyloidosis Merlini & Bellotti NEJM 2003 Sipe et al, 2012
")



75 Amyloid fibrils Misfolded FLC Small dangerous clone 1 (BMPC 7%) 53% LC only 75% l proteotoxicity structural damage λ1* λ6** Early detection of amyloid heart involvement is vital 1 Merlini & Stone, Blood. 2006; *Perfetti et al, Blood. 2012; **Comenzo et al, Br J Haematol. 1999
76 Amyloidosis: Presentation Nephrotic syndrome Refractory CHF, Arrhythmia, Heart block Orthostatic hypotension, Peripheral neuropathy Bleeding diathesis (Raccoon eyes) Factor X deficiency, liver disease GI bleeding, Gastroparesis/Dysmotility, Malabsorption Macroglossia, Shoulder pad sign, Carpal tunnel syndrome, Organomegaly Skin thickening/waxy, easy bruising




77 Diagnosis of Amyloidosis Merlini et al, Blood :
78 Amyloidosis: Work-up Biopsy Involved organs or bone marrow Fat pad, salivary glands, rectal mucosa: 50-70% success for diagnosis Echocardiography suggestive Speckled myocardium Interventricular septal thickening Distinguish from hereditary forms (10%) Evaluate for myeloma (rare)
79 AL Amyloidosis: Course Rare progression to multiple myeloma (0.4%) Poor long-term prognosis Cardiac, renal, hepatic failure, and infection Prognostic factors: circulating plasma cells, high beta-2 microglobulin, marrow plasmacytosis >10%, dominant cardiac involvement High B2M, marrow plasmacytosis: median survival 0: 54 months 1: 19 months 2: 13.5 months
80 AL Amyloidosis: Therapy Chemotherapy Dexamethasone with Dex/IFN maintenance High-dose melphalan with Auto transplantation Risky with cardiac, renal, GI involvement Dhodapkar, Blood 2004;104:3520. Skinner, Annals 2004;140:85
81 Therapy is Highly Individualized and Must be Risk-adapted Based on Cardiac Biomarkers and Response-tailored o Treatment endpoint: at least VGPR o Hematologic and cardiac response should be assessed frequently, every 1-2 cycles (or three months after ASCT) o Rapid switch if no response o Therapy can be continued for 1-2 cycles beyond best response for consolidation <VGPR Bortez if unexposed and no severe neuropathy Len, Pom 1, Benda 2 in resist. to alkyl/bortez/thal Len requires monitoring renal function New drugs, such as Ixazomib 3 1 Dispenzieri et al, Blood 2012;119 : Merlini et al, Blood. 2012;120(21) Abstr Merlini et al, Blood 2012;120(21) Abstr 731
82 Summary Spectrum of mature B-cell neoplasms/plasma cell dyscrasias Clinical manifestations: Tumor growth, marrow and tissue infiltration M-protein accumulation or infiltration Immune dysfunction Kidney and bone disease Therapy not curative, but increasingly effective