Erectile and voiding dysfunction: will stem cells solve it all?
|
|
|
- Kory Jenkins
- 5 years ago
- Views:
Transcription

1 Erectile and voiding dysfunction: will stem cells solve it all? Maarten Albersen MD PhD Dept. of Development and Regeneration Leuven University, Belgium
2 Disclosures No conflicts of interest. ED stem cell research funded by NIH, ESSM, FWO.

3 STEM CELLS symmetric division asymmetric division

4 TYPES OF STEM CELLS: pluripotent Embryonic stem cells mesoderm ectoderm endoderm muscle cartilage bone neuron glia epithelium liver cell gut epithelium lung


5 Embryonic stem cells ethical concerns tumorigenicity

6 ADULT STEM CELLS Multipotent stem cells (tissue-specific) precursor cells MSC: bone-marrow adipose tissue myoblast satellite cells? muscle cartilage bone muscle cartilage bone
7 Adult stem cells MSC: While multipotent in vitro, limited plasticity in vivo Easy to harvest with generation of high numbers of cells over time. > strong evidence base for effects may not be a result of multipotency Myoblasts: commited to one lineage, terminal differentiation shown in vivo Lenghty and difficult harvest with generation of low numbers of cells over time. Satellite cells (muscle derived stem cells): may be MSC-like and multipotent is a direct precursor of myoblast


8 abundant f- actin large ER densely packed nucleole STEM CELLS: how do they work?

")

9 The classic paradigm Stem cells would be able to engraft in the tissue where they are injected, and replace diseased/damaged/lost host tissue cells by differentiation into that specific cell type. Engraftment & differentiation In particular MSC have been shown to secrete a wide variety of bio-active molecules stimulating growth, modulating immune response, modulating extracellular matrix deposition (fibrosis) etc. Paracrine secretions Endogenous stem cells go to sites of disease, inflammation or injury to aid in the healing or repair process. Exogenous stem cells might as well be recruited to those tissues where hey are most needed. Stem cell recruitment and trafficking
10 stem cells for voiding and erectile dysfunction? allogeneic Erectile Dysfunction sphincter deficiency
11 ED
12 What animal model? ED: cavernous nerve injury (radical prostatectomy) primary outcome: intracorporeal pressure during CNS secondary outcome: nerve regeneration - prevention of secondary smooth muscle loss and fibrosis in the corpus cavernosum
13 Rationale for SC therapy Stem cells injected in the penis may replace/regenerate lost erectile smooth muscle tissue, and may enhance the process of nerve regeration.
14 ref: Albersen et al. JSM 2010 outcome: ICP


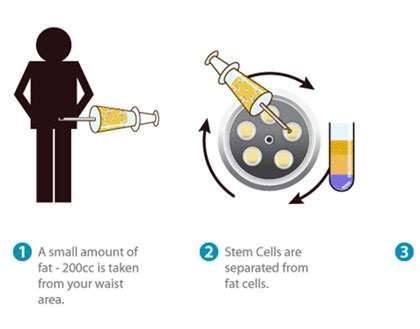

15 ADSC
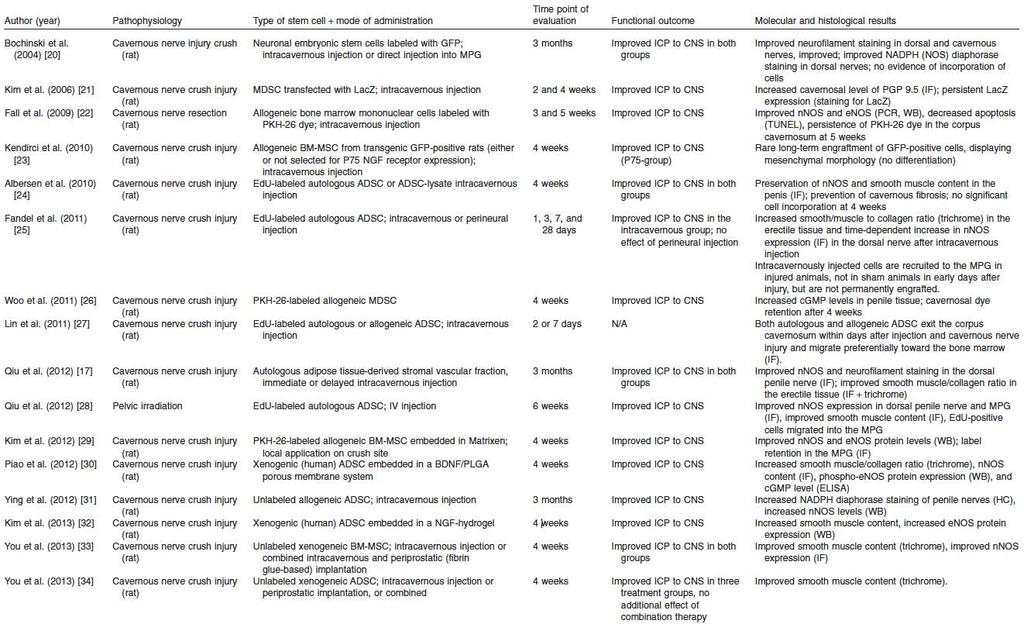
16 ref: Albersen et al. JSM 2011 ED (cavernous nerve injury)
 smooth muscle")




17 ED (cavernous nerve injury) smooth muscle no treatment fibrosis no treatment innervation no treatment b-actin ADSC ADSC ADSC nnos b-actin nnos ref: Qiu et al JSM 2012, Albersen et al. JSM 2011, Kim et al. Korean J Urol 2012,


18 ED (cavernous nerve injury) number of penile ADSC ref: Lin et al. IJIR 2010, Albersen et al. JSM 2011, Fandel et al. Eur Urol 2012
19 no engraftment: paracrine efects?
20 ref: Albersen et al. JSM 2011 ED (cavernous nerve injury)
 number of ADSC")


21 ED (cavernous nerve injury) number of ADSC detected in MPG ref: Albersen et al. JSM 2011, Fandel et al. Eur Urol 2012, Albersen et al SM 2013

22 ED (cavernous nerve injury)

23 ED (cavernous nerve injury)
24 ED (cavernous nerve injury) X!! engraftment & differentiation secretome stem cell motility and migration NO ENGRAFTMENT AND DIFFERENTIATION IN AN ACUTE INJURY MODEL OF ED paracrine signalling and homing towards the injury site are possible explanation for beneficial effect of stem cell treatment
25 SUI
26 What animal model? voiding dysfunction/urinary incontinence: Vaginal dilation (childbirth injury) Pudendal nerve injury (intrinsic sphincter deficiency) Direct cauterization trauma to sphincter (intrinsic sphincter deficiency) primary outcome: passive urethral pressure measurement (LPP) secondary outcome: striated muscle morphology restoration. Tissue integrity smooth muscle, striated muscle, extracellular matrix
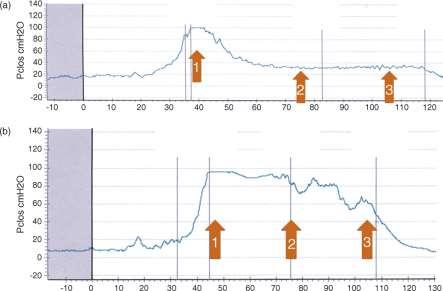
27 ref: Ahn et al. JRRD 2005 outcome: LPP
28 Rationale for SC therapy Stem cells injected in the sphincter region may either support endogenous sphincter regeneration, or even replace functionally lost skeletal muscle fibers.



29 SkMDC, satellite cells and myoblasts Does this mean SkMDC posess other properties of MSC: anti-fibrotic, anti-inflammatory?

30 SkMDC, satellite cells and myoblasts TIME
 Leak Point")

31 Animal trials (SkMDC, myoblasts) Leak Point Pressure (cmh2o) Xgal d5 Xgal d30 Xgal d30 Xgal d30


32 Animal trials (SkMDC, myoblasts)


33 Animal trials (SkMDC, myoblasts)
34 SIU (myoblasts)

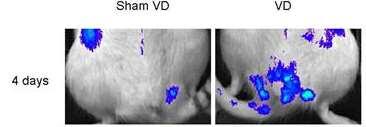
35 Animal trials (ADSC) DAPI SMA EDU (ADSC) Lin et al. Peri-urethral injection of EDU-labeled ADSC in VD rats >> retention of ADSC >> no transdifferentiation in SMC at 4 weeks. Watanabe et al. Peri-urethral injection of ADSC in PNI rats: 2 and 4 weeks after injection.




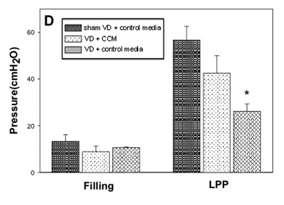
36 IV injection/secretome? IV MSC therapy improves LPP Local injection of CCM improves LPP
37 Animal trials: conclusions Tissue specific progenitors:!? X engraftment & differentiation secretome stem cell motility and migration Mesenchymal stem cells: X!!
38 Animal trials: drawbacks Care to be taken with interpretation of presence and differentiation of labeled stem/progenitor cells (several labels are transferable) Are the acute animal models a good representation of the chronic situation in humans? Is evaluation of passive pressure profiles in the urethra sufficient to conclude that the effect is to be ascribed to anything more (skeletal muscle regeneration) than bulking? Tissue-specific progenitors seem to be able to enhance autonomous or regenerate new myofiber production.


39 Clinical trials (SkMDC)


40 Clinical trials (SkMDC) incontinence score QOL score

41 Clinical trials (SkMDC)

42 Clinical trials (SkMDC)

43 Clinical trials (SkMDC)

44 Clinical trials (SkMDC)

45 Clinical trials (SkMDC)

46 Clinical trials (skeletal muscle)
47 Clinical trials (skeletal muscle)
48 SUMMARY ED: preclinical studies revealed efficacy and mechanism of action of stem cells, clinical trials underway. SUI: preclinical studies have looked at passive urethral closing/leak point pressures rather than active sphincter contraction. Novel urethral function assessment methods and more accurate models are needed. Myocytes are making their way into clinics, MSC have a long way to go.