The SAVI TM Applicator: Breast Brachytherapy Training
|
|
|
- Letitia Mills
- 6 years ago
- Views:
Transcription
1 The SAVI TM Applicator: Breast Brachytherapy Training

2 SAVI Breast Brachytherapy Greater flexibility Treats the widest array of cavity & breast sizes Enhanced performance Eliminates skin spacing restrictions Better outcomes Lowers toxicity & risk of persistent seroma Exceptional precision Sculpt dose with selective radiation Added convenience Simple, secure placement and removal


3 SAVI Product Line SAVI Applicator 6-1Mini SAVI Prep Catheter
4 SAVI Applicator Details
5 Ideal SAVI Procedure Flow Chart Pre-Implant CT Evaluation SAVI Implanted CT Simulation Treatment Planning Pre-Fraction QA and Treatment Delivery
6 SAVI Procedures Pre-Implant CT Evaluation
7 Pre-Implant CT Evaluation (w/o SPC) Performed 72 hours prior to implant 1. Obtain CT scan of breast to be treated - 3 mm slices - no gaps between slices - Patient arms up or down - Scan with breath hold if possible - Scan 2 cm superiorly and inferiorly beyond the cavity - Send CT data set to planning software 2. Have MD evaluate cavity and record data - Outline cavity margins on axial images - Determine volume (cc) of cavity - Measure the long axis (cm) and short axis (cm) - Assess the best insertion site and entry angle

8 Pre-Implant CT Evaluation 4. Using that data, determine the most appropriate SAVI applicator size using the SAVI Size Reference Chart 5. Communicate SAVI size and cavity/insertion parameters to SAVI Representative and the Physician who will implant SAVI

9 SAVI Size Reference Chart
10 Size Reference Chart
11 SAVI Procedures CT Simulation
12 CT Simulation of SAVI Implant CT Simulation is performed hours post-implant When patient arrives for the CT simulation: 1. Ask the patient for the expansion tool (surgeon should have given it to her). 2. Create an immobilization device. (e.g. Vac-Lock, alpha cradle) 3. Position patient on CT scanner and remove bandages. Patient should be supine Arms can be; above head (typical), akimbo or by her sides (if more comfortable)
13 CT Simulation of SAVI Implant 4. Place CT laser alignment marks on patient and immobilization device (for repositioning). 5. Remove the Catheter Protector from catheter #1 Insert expansion tool over catheter #1 Place in safe location to avoid damage and loss (e.g., emesis basin) The expansion tool is used for each fraction, thus insertion for planning CT provides more exact reproduction of treatment setup. Optional step: Insert a marker wire into catheter #1 (this will help identify its physical end) 6. Acquire AP and lateral scouts (print or save)
14 CT Simulation of SAVI Implant 7. Acquire planning CT data set: Use contiguous slices (e.g., no gaps) mm slice thickness Planning position must be used for treatment! Scan 2 cm superiorly and inferiorly beyond the cavity (or whole breast) 8. Evaluate implant in all three planes on CT console 9. If significant air pockets are present the device should be collapsed by the physician (left in situ), the air pockets massaged out and the device re-expanded and the CT repeated. 10. Remove expansion tool & marker wire from the SAVI (if used) 11. Replace the Catheter Protector in catheter #1
 *Record measurement on SAVI Prescription and")
15 CT Simulation of SAVI Implant 12. Measure and record* distance from skin surface to catheter handle or use the scale on catheter 1 (depth assessment) 13. Mark white ring and skin in continuous line and fill in the "clock" diagram of the SAVI template provided (rotational assessment) *Record measurement on SAVI Prescription and Treatment Summary Template
16 CT Simulation of SAVI Implant 14. Attach transfer guide tubes & measure the catheter lengths and record. (this length is NOT the treatment length) VariSource expected treatment lengths (not measured lengths) #1 length: to cm All others: to cm GammaMed lengths should be checked with the Acceptance Length wire. 15. Retain the AP & lateral scouts as reference images for pre-fraction evaluation 16. Export CT to Treatment Planning Software
17 SAVI Procedures Treatment Planning
18 Treatment Planning Contouring anatomy Identifying applicators Dose prescription and optimization DVH & Isodose Analysis
19 Contouring Anatomy Create new body structures. Consider a structure template for efficiency. SAVI = this will be the margin of the cavity in all slices PTV_Opt = this will be a 1.0 cm positive expansion of the Cavity (short for PTV for Optimization) Body = this is the surface of the skin Lung = lung-chest wall interface Chest = this surface is defined as the chest wall or pectoralis PTV_Eval = PTV_Opt minus SAVI. Also subtract Body, Lung and/or Chest as needed Other structures as needed: Cavity for air or seroma pockets outside SAVI Invag for tissue invaginating into the SAVI per MD choice
20 Case A Slice 12 Slice 15 Slice 17 Slice 22 Slice 25
21 Creating Planning Structures Create the SAVI structure using the convert isodose to structure Define PTV_Opt as 1-cm expansion of SAVI, minus Portion of expansion outside Body or Skin Portion of expansion extending into Chest and/or Lung Contour air & seroma pockets outside SAVI Name nonconforming pockets Cavity Apply 10% nonconformance rule, or Add Cavity to SAVI & redo 1-cm expansion Contour invaginated tissue PTV_Eval = PTV_Opt minus SAVI plus Invag The order of Boolean operations above is critical!
22 Contouring SAVI another way Utilize the Brush set options to 3D and Static 22

23 Draw the structure in either the Sag or Coronal view initial brush Diam 6 mm-6-1, 8 mm-8-1, & 10mm
24 24

25 Post Processing smooting level 3 - Before After 25


26 Invaginated Tissue

27 Identifying Catheters Use MPR to rotate the views until the axis of the applicator is seen clearly in 2 orthogonal views. The third view should be a head-on view of the applicator. Move through the stack of images in the head-on view from the applicator s most distal tip to the proximal end where the struts rejoin the central lumen.

28 Catheter 1 Central Lumen Catheter 1 was defined already must check that it starts in correct location Move to one of the views showing the full length of the applicator. The distal tip of #1 should be ~1.3 cm beyond the bright metal band. The final (proximal) point of #1 should be at least 1 cm past the point where the proximal ends of the struts rejoin the central channel.
29 Catheter 2, etc. Go to the head-on view window and determine which catheter is #2. Rotate the images in this window until catheter #2 is visualized fully in one of the orthogonal view windows Turn on PTV structure Insert Catheter2 defining the distal tip ~0.5 cm past the distal end of the bright band Continue to define Catheter2 in the orthogonal view that best shows the source channel Draw the applicator outside the strut Catheter3 is easiest found after locating Catheter4 which has the equatorial marker. Use the head-on view. This establishes the rotational orientation for remaining struts

30 Find Catheter 4 by adjusting Axis 30

31 Rotate to Catheter 4 31

32 Rotate to Catheter 2 32

33 Measure distance to 1 st catheter 11.3mm 33

34 Move back ruler to 2.9mm and insert 1 st catheter 34
 and insert 2 reference")

35 Move axis to ruler (2.9mm) and insert 2 reference lines on axis to mark start of delineation of peripheral catheters 35

36 Insert Catheter 2 36


37 Catheter 4 as drawn Catheter 4 as drawn Catheter 6 37

38 Source Lumens
39 Setting dwell positions Dwell positions can be set by: Manually setting start and end lengths Populating dwells inside a structure (i.e., the PTV-Opt, not the PTV-Eval) Recall that Catheter1 already has dwell times Reset all dwells to zero otherwise optimizer will start with heavy center channel loading. This will reduce your ability to modulate dose later by limiting dwells in peripheral catheters.

40 Loading Dwells Fill dwells inside PTV ONLY 40


41 Optimize Dose 41
42 Dose prescription and optimization Rx is 3.4 Gy/fx to surface of PTV_Opt (chose surface option in volume optimization window of BV) Add objective to PTV-Opt for 100% +/- 5% (e.g., 3.4 Gy +/ Gy) Dose optimization goals are as follows: PTV_Eval; 95% of volume receives 95% of prescribed dose PTV_Eval receiving 200% of dose must be < 20 cc PTV_Eval receiving 150% of dose must be < 50 cc Skin and chest wall limits met Evaluate DVH of the optimized plan Review DVH for clinical adequacy with MD With MD input, manually optimize dose to skin & chest wall Perform second check After approval by physician, follow standard operating and QA procedures for recording, documenting and exporting plan to HDR afterloader

43 Planned Case
44 DVH Analysis Comparison V90 V95 Interstitial (RTOG B-39) MammoSite (RTOG B-39) SAVI Ø 90% > 90% >90% >95% V cc 50 cc 50 cc V cc 10 cc 20 cc
45 SAVI Procedure Pre-Fraction QA and Treatment Delivery




46 Pre-Fraction QA 1. Remove all dressings 2. Position patient on CT table to match original positioning 3. Align marks on patient with CT simulator lasers 4. Measure distance from skin to central channel handle a. Compare to reference value taken at planning CT 5. Check for rotation 6. Record data on SAVI Prescription and Treatment Summary Template 6-1 and 6-1 Mini
47 Pre-Fraction QA 7. Acquire AP and lateral scouts and axial images 8. Evaluate scouts for movement or rotation of SAVI by measuring the 2, 4 and 6 markers with respect to patient anatomy. 9. If changes are noted notify Physician to re-plan/ reposition device if needed



48 Accessing Rotation How to access Rotation Look for major differences between the relative positions of the markers - AP Scouts 48


49 Accessing Rotation How to access Rotation Look for major differences between the relative positions of the markers L Lat Scouts 49

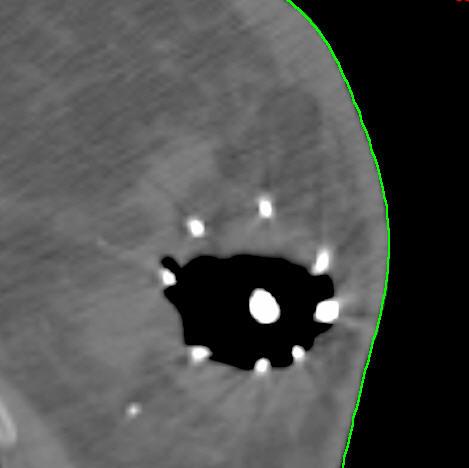
50 Scouts: Baseline & Fraction 1 Laterals Patient setup assessment Black: gap between tip and sternum is ~10 mm Patient setup assessment Black: gap between tip and sternum is ~6-7 mm (close setup) Device assessment Red: #2 is almost on center Blue: #4 at outer edge of device Yellow: 2 center have ~ 4mm gap Green: #6 is slightly inside an outer strut Fx1 Device assessment Red: #2 is almost on center (same) Blue: #4 at outer edge of device (same) Yellow: 2 center have ~ 3mm gap Green: #6 is slightly inside an outer strut (almost same)
 Green: #2 is at inner edge of ribs (slight setup difference) Device assessment Blue: #4 slightly inside the outer edge of device Yellow: #6 strut @ outer edge and ~1mm from")
 Green: #2 is at outer edge of device (same) Impression: Patient setup shows slight rotation, right-side slightly towards posterior.")
51 Scouts: Baseline & Fraction 1 AP Scouts Patient setup assessment Red: distal tip at lateral edge of ribs Green: #2 is at center of ribs Patient setup assessment Red: distal tip in middle of ribs (slight setup difference) Green: #2 is at inner edge of ribs (slight setup difference) Device assessment Blue: #4 slightly inside the outer edge of device Yellow: #6 outer edge and ~1mm from touching center Green: #2 is at outer edge of device Device assessment Blue: #4 at outer edge of device (very slight difference) Yellow: #6 outer edge and almost touching center (very slight difference) Green: #2 is at outer edge of device (same) Impression: Patient setup shows slight rotation, right-side slightly towards posterior. SAVI appears almost perfectly reproduced in AP & laterals. Slight changes in SAVI markers consistent with slight changes in patient rotation, not SAVI rotation.
52 HDR Fraction Delivery 1. In the HDR suite, position patient as for the CT Simulation 2. Remove the Catheter Protectors and store in safe location 3. Insert the Expansion Tool over the center catheter until properly engaged into the fitting of the SAVI applicator (NOTE: important for potential emergency response) 3. Obtain requisite number of transfer tubes SAVI 6-1 requires seven transfer tubes (#1-7) SAVI 8-1 requires nine transfer tubes (#1-9) SAVI 10-1 requires eleven transfer tubes (#1-11) 4. Insert proximal end of SAVI catheter #1 into the catheter connector on the distal end of transfer tube #1 5. Insert the proximal end of transfer tube #1 into the HDR unit turret s #1 opening.
 9.")
53 HDR Fraction Delivery 6. Repeat step 5 until all transfer guide tubes are connected 7. Double-check the connection numbers of the SAVI applicator, transfer guide tubes and at the turret. 8. Reposition HDR unit to maintain straightness of transfer guide tubes (as much as possible) 9. Verify each transfer guide tube connection is connected properly, and that indexer is locked
54 HDR Fraction Delivery 10. Follow SOPs for fraction delivery 11. Disconnect patient from HDR unit, disconnect transfer guide tubes from SAVI 12. Insert purple Catheter Protectors. 13. Re-bandage or dress the SAVI-skin entrance site using standard techniques

55 Inverted Strut



56 Inverted Strut Inverted Strut





57 Inverted Strut - Planned
58 Thank you!
Image based Brachytherapy- HDR applications in Partial Breast Irradiation
 Image based Brachytherapy- HDR applications in Partial Breast Irradiation Yakov Pipman, Ph.D. Long Island Jewish Medical Center Long Island Jewish Medical Center North Shore-LIJ Health System Acknowledgements
Image based Brachytherapy- HDR applications in Partial Breast Irradiation Yakov Pipman, Ph.D. Long Island Jewish Medical Center Long Island Jewish Medical Center North Shore-LIJ Health System Acknowledgements
Best Total Solutions for Breast Cancer Diagnosis & Treatment
 Best Total Solutions for Breast Cancer Diagnosis & Treatment 2015 Best Medical International, Inc. Best Medical International, Inc. 7643 Fullerton Road, Springfield, VA 22153 USA v24_08182015_web Best
Best Total Solutions for Breast Cancer Diagnosis & Treatment 2015 Best Medical International, Inc. Best Medical International, Inc. 7643 Fullerton Road, Springfield, VA 22153 USA v24_08182015_web Best
2/13/12. Brachytherapy: What, Where, Why, How, Kent A. Gifford, Ph.D. What is it? Where? Brachy- Treatment sites
 Brachytherapy: What, Where, Why, How, When Kent A. Gifford, Ph.D. What is it? Brachy- Greek word for near or short distance Notice no mention of internal Can involve sources placed in or on patient Can
Brachytherapy: What, Where, Why, How, When Kent A. Gifford, Ph.D. What is it? Brachy- Greek word for near or short distance Notice no mention of internal Can involve sources placed in or on patient Can
Clinical trials with hypo-fractionation for breast conserving therapy (BCT): Shorter overall treatment time Effective radiation treatment
: Shorter overall treatment time Effective radiation treatment") AAMD Regional Meeting, March 21st 2015 Clinical trials with hypo-fractionation for breast conserving therapy (BCT): Shorter overall treatment time Effective radiation treatment Whelan et al 2013 & Yu et
AAMD Regional Meeting, March 21st 2015 Clinical trials with hypo-fractionation for breast conserving therapy (BCT): Shorter overall treatment time Effective radiation treatment Whelan et al 2013 & Yu et
5/28/2015. AAPM Meeting 2015 Jacqueline Esthappan, PhD Washington University School of Medicine in St. Louis
 Clinical Implementation of HDR: Afterloader and Applicator Selection AAPM Meeting 2015 Jacqueline Esthappan, PhD Washington University School of Medicine in St. Louis Disclosures I will try avoid mentioning
Clinical Implementation of HDR: Afterloader and Applicator Selection AAPM Meeting 2015 Jacqueline Esthappan, PhD Washington University School of Medicine in St. Louis Disclosures I will try avoid mentioning
Multiple Metastasis Insert for the Lucy 3D QA Phantom
 Multiple Metastasis Insert for the Lucy 3D QA Phantom Tobin Hyman, MS DABR Department of Radiation Oncology, McLeod Health, Florence, SC 3120 Deming Way Middleton WI 53562-1461 USA 800-261-4446. ph 608-831-0025.
Multiple Metastasis Insert for the Lucy 3D QA Phantom Tobin Hyman, MS DABR Department of Radiation Oncology, McLeod Health, Florence, SC 3120 Deming Way Middleton WI 53562-1461 USA 800-261-4446. ph 608-831-0025.
At that time, do not reference or utilize the initial plan in any manner or study data may be compromised
 Thank you for participating in this Lung Target Delineation Project being done in conjunction with the SWOG Radiation Oncology Committee. Without your efforts, this project would not be possible. A few
Thank you for participating in this Lung Target Delineation Project being done in conjunction with the SWOG Radiation Oncology Committee. Without your efforts, this project would not be possible. A few
RPC Prostate Phantom. Guidelines for Planning and Treating the RPC IMRT Prostate Phantom. Revised November 2010
 RPC Prostate Phantom Guidelines for Planning and Treating the RPC IMRT Prostate Phantom. Revised November 2010 Credentialing for this protocol requires three steps: (1) submission of the Facility Questionaire
RPC Prostate Phantom Guidelines for Planning and Treating the RPC IMRT Prostate Phantom. Revised November 2010 Credentialing for this protocol requires three steps: (1) submission of the Facility Questionaire
Computational Verification in Interventional Radiation Oncology (Brachytherapy)
") Computational Verification in Interventional Radiation Oncology (Brachytherapy) Prof. Dr. Dimos Baltas Abteilung Medizinische Physik & Engineering Strahlenklinik Brussels, 5- December- 2014 Starkenburgring
Computational Verification in Interventional Radiation Oncology (Brachytherapy) Prof. Dr. Dimos Baltas Abteilung Medizinische Physik & Engineering Strahlenklinik Brussels, 5- December- 2014 Starkenburgring
Respiratory-phase phase correlated imaging, treatment planning and delivery Clinical Implementation. Disclosures. Session Objectives.
 Respiratory-phase phase correlated imaging, treatment planning and delivery Clinical Implementation None Disclosures Sastry Vedam Assistant Professor Department of Radiation Physics AAPM Annual Meeting
Respiratory-phase phase correlated imaging, treatment planning and delivery Clinical Implementation None Disclosures Sastry Vedam Assistant Professor Department of Radiation Physics AAPM Annual Meeting
8/2/2011. Elements of a Process Flow Trying use good planning to eliminate iterations. Thanks for contributions to this talk from
 Head and Neck Treatment Planning Disclosure Grants from Varian Medical System Thanks for contributions to this talk from Robert Foote, M.D. From M.D. Anderson Yolanda Garces, M.D. Lei Dong, Ph.D. Shelley
Head and Neck Treatment Planning Disclosure Grants from Varian Medical System Thanks for contributions to this talk from Robert Foote, M.D. From M.D. Anderson Yolanda Garces, M.D. Lei Dong, Ph.D. Shelley
Imaging/Imagine Needs for Proton Therapy: Treatment Planning. Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, CA
 Imaging/Imagine Needs for Proton Therapy: Treatment Planning Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, CA AAPM Annual Meeting Indianapolis, Aug. 07, 2013 Disclosure Software licensing agreement
Imaging/Imagine Needs for Proton Therapy: Treatment Planning Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, CA AAPM Annual Meeting Indianapolis, Aug. 07, 2013 Disclosure Software licensing agreement
DOSE SPECIFICATION AND QUALITY ASSURANCE OF RTOG PROTOCOL 95-17, A COOPERATIVE GROUP STUDY OF 192 IR BREAST IMPLANTS AS SOLE THERAPY.
 DOSE SPECIFICATION AND QUALITY ASSURANCE OF RTOG PROTOCOL 95-17, A COOPERATIVE GROUP STUDY OF 192 IR BREAST IMPLANTS AS SOLE THERAPY. W.F. Hanson 1, B. Martin 2, R. Kuske 3, D. Arthur 4, R. Rabinovitch
DOSE SPECIFICATION AND QUALITY ASSURANCE OF RTOG PROTOCOL 95-17, A COOPERATIVE GROUP STUDY OF 192 IR BREAST IMPLANTS AS SOLE THERAPY. W.F. Hanson 1, B. Martin 2, R. Kuske 3, D. Arthur 4, R. Rabinovitch
In-Room Treatment Verification Using Film and CBCT
 SAM: HDR Brachytherapy: Treatment Verification Methods In-Room Treatment Verification Using Film and CBCT Oana Craciunescu, PhD, DABR Department of Radiation Oncology Duke University Medical Center Role
SAM: HDR Brachytherapy: Treatment Verification Methods In-Room Treatment Verification Using Film and CBCT Oana Craciunescu, PhD, DABR Department of Radiation Oncology Duke University Medical Center Role
This is probably the kind of radiotherapy that you are used to delivering in your country.
 This is probably the kind of radiotherapy that you are used to delivering in your country. This slide shows images two patients, one with a T3 N2c nasopharyngeal CA and the other with a T1/2 N1/2 lung
This is probably the kind of radiotherapy that you are used to delivering in your country. This slide shows images two patients, one with a T3 N2c nasopharyngeal CA and the other with a T1/2 N1/2 lung
DIFFERENT TECHNIQUES: A SURVEY OF THE EMERGING PARTIAL BREAST IRRADIATION TECHNIQUES DISCLOSURES. Gregory K. Edmundson, M.Sc. Consulting Physicist
 DIFFERENT TECHNIQUES: A SURVEY OF THE EMERGING PARTIAL BREAST IRRADIATION TECHNIQUES Gregory K. Edmundson, M.Sc. Consulting Physicist DISCLOSURES Consulting clients include: Cianna Medical (mfr of SAVI)
DIFFERENT TECHNIQUES: A SURVEY OF THE EMERGING PARTIAL BREAST IRRADIATION TECHNIQUES Gregory K. Edmundson, M.Sc. Consulting Physicist DISCLOSURES Consulting clients include: Cianna Medical (mfr of SAVI)
Complex Treatments in Proton Therapy - Selected Topics. Martin Bues, PhD Proton Therapy M.D. Anderson Cancer Center
 Complex Treatments in Proton Therapy - Selected Topics Educational Workshop PTCOG 46, May 18-20, Wanjie, China Martin Bues, PhD Proton Therapy M.D. Anderson Cancer Center Outline Topic 1: Topic 2: Topic
Complex Treatments in Proton Therapy - Selected Topics Educational Workshop PTCOG 46, May 18-20, Wanjie, China Martin Bues, PhD Proton Therapy M.D. Anderson Cancer Center Outline Topic 1: Topic 2: Topic
SUMMARY OF CHANGES Amendment #2, Version Date: April 25, 2006
 Amendment #2, Version Date: April 25, 2006 RTOG 0321, "Phase II Trial of Combined High Dose Rate Brachytherapy and External Beam Radiotherapy for Adenocarcinoma of the Prostate" Study Chair: I-Chow Hsu,
Amendment #2, Version Date: April 25, 2006 RTOG 0321, "Phase II Trial of Combined High Dose Rate Brachytherapy and External Beam Radiotherapy for Adenocarcinoma of the Prostate" Study Chair: I-Chow Hsu,
8.0 Technical Guidelines. 8.1 Statement of treatment aim
 8.0 Technical Guidelines 8.1 Statement of treatment aim In both treatment arms, radiotherapy will consist of a conventionally fractionated radical course of treatment that aims to deliver 64 Gy in 32 fractions
8.0 Technical Guidelines 8.1 Statement of treatment aim In both treatment arms, radiotherapy will consist of a conventionally fractionated radical course of treatment that aims to deliver 64 Gy in 32 fractions
Thanks to Jeff Williamson, Mike Steinberg, James Purdy
 Thanks to Jeff Williamson, Mike Steinberg, James Purdy Radiation Therapy 1.6M new cancer cases this year in US Approximately 60% of cancer patients receive radiation therapy during the course of their
Thanks to Jeff Williamson, Mike Steinberg, James Purdy Radiation Therapy 1.6M new cancer cases this year in US Approximately 60% of cancer patients receive radiation therapy during the course of their
Treatment Quality Assurance Cone Beam Image Guided Radiation Therapy. Jean-Pierre Bissonnette, PhD, MCCPM
 Treatment Quality Assurance Cone Beam Image Guided Radiation Therapy Jean-Pierre Bissonnette, PhD, MCCPM Disclosure Work supported, in part, by Elekta Oncology Systems Commercial Interest in Penta-Guide
Treatment Quality Assurance Cone Beam Image Guided Radiation Therapy Jean-Pierre Bissonnette, PhD, MCCPM Disclosure Work supported, in part, by Elekta Oncology Systems Commercial Interest in Penta-Guide
An updates on ART for prostate, pancreas and breast
 An updates on ART for prostate, pancreas and breast X. Allen Li Medical College of Wisconsin TH-E-137, AAPM Edu Course, Aug. 8, 2013 Acknowledgement Ergun Ahunbay, Ph.D Guangpei Chen, Ph.D Feng Liu, Ph.D
An updates on ART for prostate, pancreas and breast X. Allen Li Medical College of Wisconsin TH-E-137, AAPM Edu Course, Aug. 8, 2013 Acknowledgement Ergun Ahunbay, Ph.D Guangpei Chen, Ph.D Feng Liu, Ph.D
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/76501/ This is the author s version of a work that was submitted to / accepted
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/76501/ This is the author s version of a work that was submitted to / accepted
RADIATION ONCOLOGY RESIDENCY PROGRAM Competency Evaluation of Resident
 Resident s Name: RADIATION ONCOLOGY RESIDENCY PROGRAM Competency Evaluation of Resident Rotation: PHYS 705: Clinical Rotation 3 Inclusive dates of rotation: Aug. 25, 2015 Feb. 25, 2016 Director or Associate
Resident s Name: RADIATION ONCOLOGY RESIDENCY PROGRAM Competency Evaluation of Resident Rotation: PHYS 705: Clinical Rotation 3 Inclusive dates of rotation: Aug. 25, 2015 Feb. 25, 2016 Director or Associate
Integrating the MR-Linac into Radiation Therapy Practice
 Integrating the MR-Linac into Radiation Therapy Practice Mikki Campbell MRT(T), MHE Winnie Li MRT(T), MSc UTDRO Evening Journal Club MR-Linac: From Prototype to Clinical January 24, 2019 Objectives To
Integrating the MR-Linac into Radiation Therapy Practice Mikki Campbell MRT(T), MHE Winnie Li MRT(T), MSc UTDRO Evening Journal Club MR-Linac: From Prototype to Clinical January 24, 2019 Objectives To
Optimizing Treatment Planning Process in Clinical Enviroment
 Optimizing Treatment Planning Process in Clinical Enviroment Wenzheng Feng 12 (1) Columbia University Medical Center, New York, NY (2) Bayhealth Medical Center, Dover, DE Objectives: 1. Be familiar with
Optimizing Treatment Planning Process in Clinical Enviroment Wenzheng Feng 12 (1) Columbia University Medical Center, New York, NY (2) Bayhealth Medical Center, Dover, DE Objectives: 1. Be familiar with
Brachytherapy. Linda Poplawski. Graduate Program of Medical Physics Duke University. Date: Approved: Oana Craciunescu, Supervisor.
 Evaluating Dose Summation in Gynecological Brachytherapy by Linda Poplawski Graduate Program of Medical Physics Duke University Date: Approved: Oana Craciunescu, Supervisor Junzo Chino Joseph Lo Thesis
Evaluating Dose Summation in Gynecological Brachytherapy by Linda Poplawski Graduate Program of Medical Physics Duke University Date: Approved: Oana Craciunescu, Supervisor Junzo Chino Joseph Lo Thesis
Integrated on-board CBCT-US imaging system for soft tissue IGRT and real-time intra-fraction monitoring
 Integrated on-board CBCT-US imaging system for soft tissue IGRT and real-time intra-fraction monitoring John Wong Radiation Oncology and Molecular Radiation Sciences Johns Hopkins University School of
Integrated on-board CBCT-US imaging system for soft tissue IGRT and real-time intra-fraction monitoring John Wong Radiation Oncology and Molecular Radiation Sciences Johns Hopkins University School of
Brachytherapy Source Calibration
 Brachytherapy Source Calibration HDR and LDR Iridium, Iodine, Palladium, Cesium, and Strontium MAX 4000 Electrometer and HDR 1000 Plus Well Chamber. Calibration of individual and multiple isotopes Outstanding
Brachytherapy Source Calibration HDR and LDR Iridium, Iodine, Palladium, Cesium, and Strontium MAX 4000 Electrometer and HDR 1000 Plus Well Chamber. Calibration of individual and multiple isotopes Outstanding
MRI-Guided On-line Adaptive Radiotherapy The UCLA Physics Experience. Disclosures 8/3/2016
 MRI-Guided On-line Adaptive Radiotherapy The UCLA Physics Experience James Lamb, Nzhde Agazaryan, Minsong Cao, Mitch Kamrava, Percy Lee, Daniel Low, David Thomas, Yingli Yang Department of Radiation Oncology
MRI-Guided On-line Adaptive Radiotherapy The UCLA Physics Experience James Lamb, Nzhde Agazaryan, Minsong Cao, Mitch Kamrava, Percy Lee, Daniel Low, David Thomas, Yingli Yang Department of Radiation Oncology
Initial Certification
 Initial Certification Therapeutic Medical Physics (TMP) Content Guide Part 2 Content Guide and Sample Questions PLEASE NOTE: List of Constants and Physical Values for Use on the Part 2 Physics Exams The
Initial Certification Therapeutic Medical Physics (TMP) Content Guide Part 2 Content Guide and Sample Questions PLEASE NOTE: List of Constants and Physical Values for Use on the Part 2 Physics Exams The
YUKON DES. PEARL surface. Drug Eluting Stent System. Coronary Stent System for individual drug coating application. Stent coating machine
 YUKON DES PEARL surface Drug Eluting Stent System Coronary Stent System for individual drug coating application Stent coating machine Free choice of drug Individual dosage No polymer coating Sterile coating
YUKON DES PEARL surface Drug Eluting Stent System Coronary Stent System for individual drug coating application Stent coating machine Free choice of drug Individual dosage No polymer coating Sterile coating
Needle Loading. Seed Sterilization. Shielding. Seed Handling. SeedVac Seed Slider. Seed Sterilization and Sorting Tray Seed Sterilization Pill Box
 Prepare Prostate Brachytherapy treatments fast and with minimal exposure. Standard Imaging can provide you with complete kits that easily provide everything needed to start a prostate implant program.
Prepare Prostate Brachytherapy treatments fast and with minimal exposure. Standard Imaging can provide you with complete kits that easily provide everything needed to start a prostate implant program.
3/6/2017 TOMOSYNTHESIS GUIDED BREAST BIOPSY LEARNING OBJECTIVES DISCLOSURES
 TOMOSYNTHESIS GUIDED BREAST BIOPSY Amy Kerger, D.O. Assistant Professor The Ohio State Wexner Medical Center Stefanie Spielman Comprehensive Breast Center LEARNING OBJECTIVES What is the difference between
TOMOSYNTHESIS GUIDED BREAST BIOPSY Amy Kerger, D.O. Assistant Professor The Ohio State Wexner Medical Center Stefanie Spielman Comprehensive Breast Center LEARNING OBJECTIVES What is the difference between
Assessing dose variance from immobilization devices in VMAT head and neck treatment planning: A retrospective case study analysis
 Assessing dose variance from immobilization devices in VMAT head and neck treatment planning: A retrospective case study analysis Alyssa Olson, B.S., R.T.(T), Kristine Phillips, B.S., R.T.(T), Tamara Eng
Assessing dose variance from immobilization devices in VMAT head and neck treatment planning: A retrospective case study analysis Alyssa Olson, B.S., R.T.(T), Kristine Phillips, B.S., R.T.(T), Tamara Eng
DESIGN OF AN ANTHROPOMORPHIC INTENSITY MODULATED RADIATION THERAPY QUALITY ASSURANCE PHANTOM
 DESIGN OF AN ANTHROPOMORPHIC INTENSITY MODULATED RADIATION THERAPY QUALITY ASSURANCE PHANTOM Dee-Ann Radford, David S. Followill, Peter A. Balter, William F. Hanson Department of Radiation Physics The
DESIGN OF AN ANTHROPOMORPHIC INTENSITY MODULATED RADIATION THERAPY QUALITY ASSURANCE PHANTOM Dee-Ann Radford, David S. Followill, Peter A. Balter, William F. Hanson Department of Radiation Physics The
SBRT LUNG CANCER CLINICAL PATHWAY
 SBRT LUNG CANCER CLINICAL PATHWAY Final Draft March 2015 Cancer Clinical Performance Group Radiation Oncology SBRT Workgroup Membership: Rex Hoffman, MD, Clinical Lead, Disney Family Cancer Center (Burbank,
SBRT LUNG CANCER CLINICAL PATHWAY Final Draft March 2015 Cancer Clinical Performance Group Radiation Oncology SBRT Workgroup Membership: Rex Hoffman, MD, Clinical Lead, Disney Family Cancer Center (Burbank,
High performance comes easily
 High performance comes easily Philips MX 16-slice CT Easy from any The CT solution Your days may not be getting any easier, but now your CT solution is. The remarkably easy-to-use Philips MX 16-slice CT
High performance comes easily Philips MX 16-slice CT Easy from any The CT solution Your days may not be getting any easier, but now your CT solution is. The remarkably easy-to-use Philips MX 16-slice CT
SPECIFICATION. High Dose Rate Brachytherapy Equipment Package
 SPECIFICATION High Dose Rate Brachytherapy Equipment Package 1. Scope This specification describes the equipment requirements for a new high dose rate brachytherapy service required at the Hospital General
SPECIFICATION High Dose Rate Brachytherapy Equipment Package 1. Scope This specification describes the equipment requirements for a new high dose rate brachytherapy service required at the Hospital General
Disclosures 7/31/2017. Clinical Impact and Applications of 4D Imaging (in RT)
") Clinical Impact and Applications of 4D Imaging (in RT) Geoff Hugo, Ph.D. Virginia Commonwealth University Washington University School of Medicine gdhugo@wustl.edu Disclosures Employee of Virginia Commonwealth
Clinical Impact and Applications of 4D Imaging (in RT) Geoff Hugo, Ph.D. Virginia Commonwealth University Washington University School of Medicine gdhugo@wustl.edu Disclosures Employee of Virginia Commonwealth
Automated Breast Volumes. Simplified.
 www.siemens.com/ultrasound Automated Breast Volumes. Simplified. ACUSON S2000 Automated Breast Volume Scanner (ABVS) Answers for life. Automated Breast Volumes. Simplified. ACUSON S2000 Automated Breast
www.siemens.com/ultrasound Automated Breast Volumes. Simplified. ACUSON S2000 Automated Breast Volume Scanner (ABVS) Answers for life. Automated Breast Volumes. Simplified. ACUSON S2000 Automated Breast
Optimizing Adaptive Workflows Using RapidPlan at the Beatson West of Scotland Cancer Centre
 Case Study RapidPlan Adaptive Workflows Optimizing Adaptive Workflows Using RapidPlan at the Beatson West of Scotland Cancer Centre Introduction Adaptive radiotherapy is the practice of adapting to changes
Case Study RapidPlan Adaptive Workflows Optimizing Adaptive Workflows Using RapidPlan at the Beatson West of Scotland Cancer Centre Introduction Adaptive radiotherapy is the practice of adapting to changes
Strategies for Adaptive RT
 Strategies for Adaptive RT Olga L. Green Disclosures Honoraria and travel grants from ViewRay, Inc. 1 Learning Objectives What is ART? What is needed to implement real-time, online ART in the clinic? Example
Strategies for Adaptive RT Olga L. Green Disclosures Honoraria and travel grants from ViewRay, Inc. 1 Learning Objectives What is ART? What is needed to implement real-time, online ART in the clinic? Example
SPECIFICATION. High Dose Rate Brachytherapy Equipment Package
 1. Scope SPECIFICATION High Dose Rate Brachytherapy Equipment Package This specification describes the equipment requirements for a new high dose rate brachytherapy service required at National Cancer
1. Scope SPECIFICATION High Dose Rate Brachytherapy Equipment Package This specification describes the equipment requirements for a new high dose rate brachytherapy service required at National Cancer
Practical Workflow and the Cost of Adaptive Therapy. Rojano Kashani, Ph.D., DABR Washington University School of Medicine March 7, 2015
 Practical Workflow and the Cost of Adaptive Therapy Rojano Kashani, Ph.D., DABR Washington University School of Medicine March 7, 2015 Disclosures Travel expenses paid by ViewRay Inc. for on-site software
Practical Workflow and the Cost of Adaptive Therapy Rojano Kashani, Ph.D., DABR Washington University School of Medicine March 7, 2015 Disclosures Travel expenses paid by ViewRay Inc. for on-site software
CT Cystogram CT Pelvis WO
 CT Cystogram CT Pelvis WO Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle,
CT Cystogram CT Pelvis WO Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle,
MR Guided Radiation Therapy: ViewRay System Sasa Mutic, Ph.D.
 MR Guided Radiation Therapy: ViewRay System Sasa Mutic, Ph.D. Conflict of Interest Statement Shareholder - ViewRay Inc. Clinical advisory board - ViewRay Inc. Research and service - ViewRay Inc. Learning
MR Guided Radiation Therapy: ViewRay System Sasa Mutic, Ph.D. Conflict of Interest Statement Shareholder - ViewRay Inc. Clinical advisory board - ViewRay Inc. Research and service - ViewRay Inc. Learning
The application of error reduction QA philosophy in HDR brachytherapy
 The application of error reduction QA philosophy in HDR brachytherapy Bruce Thomadsen University of Wisconsin - Madison Learning Objectives Learning objectives: To understand 1. The problem with the current
The application of error reduction QA philosophy in HDR brachytherapy Bruce Thomadsen University of Wisconsin - Madison Learning Objectives Learning objectives: To understand 1. The problem with the current
Brachytherapy applicators. and accessories
 Brachytherapy applicators and accessories Introduction At Nucletron, we believe that our solutions, services and extensive knowledge of precisely targeted radiotherapy can play a vital role in the successful
Brachytherapy applicators and accessories Introduction At Nucletron, we believe that our solutions, services and extensive knowledge of precisely targeted radiotherapy can play a vital role in the successful
ViewRay Experience. Sasa Mutic, Ph.D. Washington University School of Medicine
 ViewRay Experience Sasa Mutic, Ph.D. Washington University School of Medicine You can observe a lot, just by watching -Yogi Berra Does organ motion matter? A slide often used to illustrate RT capabilities
ViewRay Experience Sasa Mutic, Ph.D. Washington University School of Medicine You can observe a lot, just by watching -Yogi Berra Does organ motion matter? A slide often used to illustrate RT capabilities
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment In-Service Presentation Acoustic Pulse Thrombolysis treatment is a minimally invasive system for accelerating thrombus dissolution. FORWARD-LOOKING STATEMENT This
Acoustic Pulse Thrombolysis Treatment In-Service Presentation Acoustic Pulse Thrombolysis treatment is a minimally invasive system for accelerating thrombus dissolution. FORWARD-LOOKING STATEMENT This
Brachytherapy Practice Problems EXTRA
 Brachytherapy Practice Problems EXTRA 1. 100 mci decays to 12.5 mci in days, if the half-life is 17d. a. 170 b. 136 c. 85 d. 51 e. 25 2. A radionuclide has a half-life of 74 d. The activity after 370 days
Brachytherapy Practice Problems EXTRA 1. 100 mci decays to 12.5 mci in days, if the half-life is 17d. a. 170 b. 136 c. 85 d. 51 e. 25 2. A radionuclide has a half-life of 74 d. The activity after 370 days
Going Clinical with the Accuray Radixact System. The Montefiore Experience
 Going Clinical with the Accuray Radixact System The Montefiore Experience Disclaimer The views expressed in the presentation are those of the presenters and do not necessarily reflect the views or policies
Going Clinical with the Accuray Radixact System The Montefiore Experience Disclaimer The views expressed in the presentation are those of the presenters and do not necessarily reflect the views or policies
Ingenia MR-RT. MR Systems. The comprehensive MR-sim solution to fit your planning
 Ingenia MR-RT MR Systems The comprehensive MR-sim solution to fit your planning Table of contents Experience the difference MRI makes 3 A comprehensive MR-sim solution 4 Position with precision 6 See clearly
Ingenia MR-RT MR Systems The comprehensive MR-sim solution to fit your planning Table of contents Experience the difference MRI makes 3 A comprehensive MR-sim solution 4 Position with precision 6 See clearly
Leksell. Vantage Stereotactic System. Advancing stereotactic neurosurgery
 Leksell Vantage Stereotactic System Advancing stereotactic neurosurgery Innovation built on strong foundations Since the founding of our company by Lars Leksell more than 45 years ago, Elekta has delivered
Leksell Vantage Stereotactic System Advancing stereotactic neurosurgery Innovation built on strong foundations Since the founding of our company by Lars Leksell more than 45 years ago, Elekta has delivered
Percutaneous Spinal Injections problem presentation for HW1
 Percutaneous Spinal Injections problem presentation for HW1 Gabor Fichtinger, PhD Director of Engineering, Associate Research Professor of Computer Science and Radiology NSF-Funded Funded Engineering Research
Percutaneous Spinal Injections problem presentation for HW1 Gabor Fichtinger, PhD Director of Engineering, Associate Research Professor of Computer Science and Radiology NSF-Funded Funded Engineering Research
R/F. Experiences Using SONIALVISION safire and the Utility of Tomosynthesis. 1. Introduction. 2. Basics of Tomosynthesis.
 R/F Experiences Using SONIALVISION safire and the Utility of Tomosynthesis Radiology Division, Dokkyo Medical University Koshigaya Hospital Masahiro Nakajima Mr. Masahiro Nakajima 1. Introduction The hospital
R/F Experiences Using SONIALVISION safire and the Utility of Tomosynthesis Radiology Division, Dokkyo Medical University Koshigaya Hospital Masahiro Nakajima Mr. Masahiro Nakajima 1. Introduction The hospital
IMRT PHANTOMS CIRS IMRT HOMOGENEOUS PHANTOM CIRS IMRT PHANTOMS C-1
 IRS IMRT PHANTOMS IMRT PHANTOMS The IRS IMRT Phantoms for Film and Ion hamber Dosimetry are designed to address the complex issues surrounding commissioning and comparison of treatment planning systems
IRS IMRT PHANTOMS IMRT PHANTOMS The IRS IMRT Phantoms for Film and Ion hamber Dosimetry are designed to address the complex issues surrounding commissioning and comparison of treatment planning systems
Adaptive Re-planning for Lung RT with Multi-targets
 Adaptive Re-planning for Lung RT with Multi-targets Feng Liu, An Tai, Ergun Ahunbay, Elizabeth Gore, Candice Johnstone, X. Allen Li Medical College of Wisconsin NCC AAMP, Madison, Oct. 11, 2013 Motivation:
Adaptive Re-planning for Lung RT with Multi-targets Feng Liu, An Tai, Ergun Ahunbay, Elizabeth Gore, Candice Johnstone, X. Allen Li Medical College of Wisconsin NCC AAMP, Madison, Oct. 11, 2013 Motivation:
LDR Real-time Prostate Solution Dedicated, Automated Seed Brachytherapy. Powerful solutions from the authority on brachytherapy
 LDR Real-time Prostate Solution Dedicated, Automated Seed Brachytherapy Powerful solutions from the authority on brachytherapy LDR Real-time Prostate Solution Low Dose Rate (LDR) brachytherapy is a widely
LDR Real-time Prostate Solution Dedicated, Automated Seed Brachytherapy Powerful solutions from the authority on brachytherapy LDR Real-time Prostate Solution Low Dose Rate (LDR) brachytherapy is a widely
Do You Know? Best Medical
 Which of the following companies is still the most reliable and trusted source of Iodine-125 and Palladium-103 seeds for prostate brachytherapy? Best Iodine-125 Seed Best Palladium-103 Seed 5 mm spacer
Which of the following companies is still the most reliable and trusted source of Iodine-125 and Palladium-103 seeds for prostate brachytherapy? Best Iodine-125 Seed Best Palladium-103 Seed 5 mm spacer
Prostate Brachytherapy
 Prostate Brachytherapy Seed Handling and Needle Loading Instruments Fast with Minimal Exposure Check with us FIRST for all your seed handling and calibration needs. TM www.standardimaging.com SeedVac Needle
Prostate Brachytherapy Seed Handling and Needle Loading Instruments Fast with Minimal Exposure Check with us FIRST for all your seed handling and calibration needs. TM www.standardimaging.com SeedVac Needle
2017 ACR Computed Tomography Quality Control Manual FAQS
 Updated 11-15-2017 2017 ACR Computed Tomography Quality Control Manual FAQS Q. The updated 2017 ACR Computed Tomography Quality Control Manual has been released. (Visit www.acr.org/education/education-catalog.)
Updated 11-15-2017 2017 ACR Computed Tomography Quality Control Manual FAQS Q. The updated 2017 ACR Computed Tomography Quality Control Manual has been released. (Visit www.acr.org/education/education-catalog.)
UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A WRITTEN DIRECTIVE SURROGATE FOR PHYSICIAN REAL-TIME IGRT APPROVAL
 1 UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A WRITTEN DIRECTIVE SURROGATE FOR PHYSICIAN REAL-TIME IGRT APPROVAL A Research Project Report Submitted in Partial Fulfillment of the Requirements for
1 UNIVERSITY OF WISCONSIN-LA CROSSE Graduate Studies A WRITTEN DIRECTIVE SURROGATE FOR PHYSICIAN REAL-TIME IGRT APPROVAL A Research Project Report Submitted in Partial Fulfillment of the Requirements for
A comparison between hydrogel spacer and endorectal balloon: An analysis of intrafraction prostate motion during proton therapy
 Received: 28 October 2016 Revised: 13 December 2016 Accepted: 8 January 2017 DOI: 10.1002/acm2.12051 RADIATION ONCOLOGY PHYSICS A comparison between hydrogel spacer and endorectal balloon: An analysis
Received: 28 October 2016 Revised: 13 December 2016 Accepted: 8 January 2017 DOI: 10.1002/acm2.12051 RADIATION ONCOLOGY PHYSICS A comparison between hydrogel spacer and endorectal balloon: An analysis
Evaluation of Dynamic Conformal Arc Therapy for Treatment of Lung and Liver
 Evaluation of Dynamic Conformal Arc Therapy for Treatment of Lung and Liver Sotiri Stathakis, PhD, DABR Disclosure ELEKTA Monaco research support I do not have a financial interest in any company or product
Evaluation of Dynamic Conformal Arc Therapy for Treatment of Lung and Liver Sotiri Stathakis, PhD, DABR Disclosure ELEKTA Monaco research support I do not have a financial interest in any company or product
experienced. focused. evolving. just like you.
 experienced. focused. evolving. just like you. CONTROL MODULE Together, we re changing the outcome Over the past 17 years, we ve partnered with clinicians to achieve some remarkable firsts in breast cancer
experienced. focused. evolving. just like you. CONTROL MODULE Together, we re changing the outcome Over the past 17 years, we ve partnered with clinicians to achieve some remarkable firsts in breast cancer
CT QA SOLUTIONS. Ensure Accurate Screening, Diagnosis and Monitoring ACCREDITATION CT IMAGE QUALITY QA CTDI CT CHARACTERIZATION CT PERFUSION QA
 CT QA SOLUTIONS Ensure Accurate Screening, Diagnosis and Monitoring ACCREDITATION CT IMAGE QUALITY QA CTDI CT CHARACTERIZATION CT PERFUSION QA COMPLETE CT QA With more than 40 years of experience in the
CT QA SOLUTIONS Ensure Accurate Screening, Diagnosis and Monitoring ACCREDITATION CT IMAGE QUALITY QA CTDI CT CHARACTERIZATION CT PERFUSION QA COMPLETE CT QA With more than 40 years of experience in the
CT procedure with needle guidance for heptatocellular carcinoma
 CT procedure with needle guidance for heptatocellular carcinoma Philips EPIQ image fusion and navigation case study Hepatocellular carcinoma (HCC) is a common condition worldwide. There has been increasing
CT procedure with needle guidance for heptatocellular carcinoma Philips EPIQ image fusion and navigation case study Hepatocellular carcinoma (HCC) is a common condition worldwide. There has been increasing
Comprehensive Solutions
 Comprehensive Solutions in Ultrasound-guided Breast Biopsy ATEC Vacuum-assisted Breast Biopsy System Celero Vacuum-assisted, Spring loaded Core Breast Biopsy Device Tru-Core II Spring loaded Core Breast
Comprehensive Solutions in Ultrasound-guided Breast Biopsy ATEC Vacuum-assisted Breast Biopsy System Celero Vacuum-assisted, Spring loaded Core Breast Biopsy Device Tru-Core II Spring loaded Core Breast
Integrated planning, navigation and robotic targeting for tumor ablation
 Integrated planning, navigation and robotic targeting for tumor ablation Tumor ablation Current practice Today, clinicians plan their interventional oncology procedures by viewing 2 dimensional CT slices,
Integrated planning, navigation and robotic targeting for tumor ablation Tumor ablation Current practice Today, clinicians plan their interventional oncology procedures by viewing 2 dimensional CT slices,
Target point correction optimized based on the dose distribution of each fraction in daily IGRT
 Journal of Physics: Conference Series OPEN ACCESS Target point correction optimized based on the dose distribution of each fraction in daily IGRT To cite this article: Markus Stoll et al 2014 J. Phys.:
Journal of Physics: Conference Series OPEN ACCESS Target point correction optimized based on the dose distribution of each fraction in daily IGRT To cite this article: Markus Stoll et al 2014 J. Phys.:
Making the difference
 Veradius Unity Surgery Making the difference with Live Image Guidance Enjoy straightforward surgical imaging Key advantages Transform your surgical procedures with a system as easy to use as a tablet.
Veradius Unity Surgery Making the difference with Live Image Guidance Enjoy straightforward surgical imaging Key advantages Transform your surgical procedures with a system as easy to use as a tablet.
Considerations and Issues in Electronic Charting for Brachytherapy
 Considerations and Issues in Electronic Charting for Brachytherapy A report from the work group of TG262 Susan Richardson, Ph.D. Why? The American Reinvestment & Recovery Act (ARRA) was enacted in 2009.
Considerations and Issues in Electronic Charting for Brachytherapy A report from the work group of TG262 Susan Richardson, Ph.D. Why? The American Reinvestment & Recovery Act (ARRA) was enacted in 2009.
I M A G E G U I D E D R A D I A T I O N T H E R A P Y. Elekta XVI. Inspiring clinical confidence
 I M A G E G U I D E D R A D I A T I O N T H E R A P Y Elekta XVI Inspiring clinical confidence 1 New levels of precision and accuracy Tumor target motion is a significant factor in inhibiting increasing
I M A G E G U I D E D R A D I A T I O N T H E R A P Y Elekta XVI Inspiring clinical confidence 1 New levels of precision and accuracy Tumor target motion is a significant factor in inhibiting increasing
Merit Medical s Innovative Family. of Vascular Access Products. A Great Introduction
 Merit Medical s Innovative Family of Vascular Access Products A Great Introduction Sheath Introducers The Prelude family of sheath introducers is a comprehensive product line offering excellent transitions,
Merit Medical s Innovative Family of Vascular Access Products A Great Introduction Sheath Introducers The Prelude family of sheath introducers is a comprehensive product line offering excellent transitions,
Clinical Experience with Knowledge-Based Planning. Lindsey Olsen, M.S. Washington University in St. Louis
 Clinical Experience with Knowledge-Based Planning Lindsey Olsen, M.S. Washington University in St. Louis Disclosures Speaker Agreement with Varian Medical Systems License Agreement with Varian Medical
Clinical Experience with Knowledge-Based Planning Lindsey Olsen, M.S. Washington University in St. Louis Disclosures Speaker Agreement with Varian Medical Systems License Agreement with Varian Medical
CT Guided Electromagnetic Navigational Bronchoscopy
 CT Guided Electromagnetic Navigational Bronchoscopy Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Chief Thoracic Surgery, Chief Medical Officer
CT Guided Electromagnetic Navigational Bronchoscopy Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Chief Thoracic Surgery, Chief Medical Officer
Trusted Performance. Smart Investment. 80 detector row Ultra Helical CT
 TM Trusted Performance. Smart Investment. 80 detector row Ultra Helical CT 2 High performance, highly economical Increased productivity and patient safety Maximum clinical capabilities Are you looking
TM Trusted Performance. Smart Investment. 80 detector row Ultra Helical CT 2 High performance, highly economical Increased productivity and patient safety Maximum clinical capabilities Are you looking
AAPM TG-275: Live Demonstration of Chart Checks
 AAPM TG-275: Live Demonstration of Chart Checks EBRT Plan Review: RayStation and Mosaiq Stephanie Parker, MS, DABR, CSSGB Conflicts of Interest unone Systems Acknowledgements ucurtis Whiddon, Ph.D. ushiva
AAPM TG-275: Live Demonstration of Chart Checks EBRT Plan Review: RayStation and Mosaiq Stephanie Parker, MS, DABR, CSSGB Conflicts of Interest unone Systems Acknowledgements ucurtis Whiddon, Ph.D. ushiva
Curriculum For Computer Aided Design (CAD) Operator Leather Sector (Duration of Course Six Months) Code: VF53S001
 Operator Leather Sector (Duration of Course Six Months) Code: VF53S001") Curriculum For Computer Aided Design (CAD) Operator Leather Sector (Duration of Course Six Months) Code: VF53S001 Page 1 Introduction Template Overall objective of course To provide the basic skill in
Curriculum For Computer Aided Design (CAD) Operator Leather Sector (Duration of Course Six Months) Code: VF53S001 Page 1 Introduction Template Overall objective of course To provide the basic skill in
Disclosures. Outline 8/2/2017. Emerging Technologies for IORT: Unidirectional Planar Brachytherapy Sources. Julius V Turian PhD 8/2/2017
 Emerging Technologies for IORT: Unidirectional Planar Brachytherapy Sources 8/2/2017 59 th AAPM Annual Meeting Denver CO Session Number: WE-B-702-04 Disclosures Rush University is participating in a pancreatic
Emerging Technologies for IORT: Unidirectional Planar Brachytherapy Sources 8/2/2017 59 th AAPM Annual Meeting Denver CO Session Number: WE-B-702-04 Disclosures Rush University is participating in a pancreatic
Stereotactic Body Radiation Therapy: Planning and Delivery
 Stereotactic Body Radiation Therapy: Planning and Delivery Yong Yang, Ph.D. Department of Radiation Oncology Stanford University 6 AAPM Therapy Educational Course Stanford Radiation Physics Lei Xing, Ph.D.
Stereotactic Body Radiation Therapy: Planning and Delivery Yong Yang, Ph.D. Department of Radiation Oncology Stanford University 6 AAPM Therapy Educational Course Stanford Radiation Physics Lei Xing, Ph.D.
Process Mapping. Acknowledgements 7/21/2014. Disclosures
 Process Mapping Jatinder R Palta, PhD, FAAPM, FASTRO Professor and Chair Medical Physics, VCU Chief Physicist, VHA Radiation Oncology Richmond, Virginia Acknowledgements Derek Brown, PhD University of
Process Mapping Jatinder R Palta, PhD, FAAPM, FASTRO Professor and Chair Medical Physics, VCU Chief Physicist, VHA Radiation Oncology Richmond, Virginia Acknowledgements Derek Brown, PhD University of
Surgical Coordinating Center for CLEAR III The University of Chicago Chicago, Illinois
 Surgical Protocol for External Ventricular Catheter (EVD) Placement for CLEAR III Trial Surgical Coordinating Center for CLEAR III The University of Chicago Chicago, Illinois June 17, 2009 General Principles
Surgical Protocol for External Ventricular Catheter (EVD) Placement for CLEAR III Trial Surgical Coordinating Center for CLEAR III The University of Chicago Chicago, Illinois June 17, 2009 General Principles
IMAGE GUIDANCE DOSES IN RADIOTHERAPY. Scott Crowe
 IMAGE GUIDANCE DOSES IN RADIOTHERAPY Scott Crowe IMAGING DOSE ALARA requires that imaging dose is managed and optimised Imaging dose presents an increased risk for paediatric patients Increased effective
IMAGE GUIDANCE DOSES IN RADIOTHERAPY Scott Crowe IMAGING DOSE ALARA requires that imaging dose is managed and optimised Imaging dose presents an increased risk for paediatric patients Increased effective
8: IV/SQ Maintenance
 Section 8: IV/SQ Maintenance Section Author(s): abalmforth & wbethurum Field Guide Section 8: IV/SQ Maintenance 1 Section 8: IV & SQ Maintenance 2 Section 8: IV/SW Maintenance Field Guide Section Contents
Section 8: IV/SQ Maintenance Section Author(s): abalmforth & wbethurum Field Guide Section 8: IV/SQ Maintenance 1 Section 8: IV & SQ Maintenance 2 Section 8: IV/SW Maintenance Field Guide Section Contents
Fluoroscan Insight-FD Mini C-arm System Redefining Mini C-arm Technology
 EXTREMITY C-ARM IMAGING Fluoroscan Insight-FD Mini C-arm System Redefining Mini C-arm Technology 1800 Williamson Ct. Louisville, Kentucky 40223 USA 800-923-8413 502-244-6345 FAX: 502-244-0369 www.dremed.com
EXTREMITY C-ARM IMAGING Fluoroscan Insight-FD Mini C-arm System Redefining Mini C-arm Technology 1800 Williamson Ct. Louisville, Kentucky 40223 USA 800-923-8413 502-244-6345 FAX: 502-244-0369 www.dremed.com
The Optimization of Inverse Planning and IMRT
 The Optimization of Inverse Planning and IMRT James M. Galvin, D.Sc. Ying Xiao, Ph.D. Yan Chen, Ph.D. Greg Bednarz, Ph.D. Darek Michalski, Ph.D. Yair Censor, Ph.D. Chris Houser, B.S. Murshed Hossain, PhD
The Optimization of Inverse Planning and IMRT James M. Galvin, D.Sc. Ying Xiao, Ph.D. Yan Chen, Ph.D. Greg Bednarz, Ph.D. Darek Michalski, Ph.D. Yair Censor, Ph.D. Chris Houser, B.S. Murshed Hossain, PhD
Breast Reconstruction Using Patients Own Tissue Based on CT Angiography and 3-D Surface Scanning
 Breast Reconstruction Using Patients Own Tissue Based on CT Angiography and 3-D Surface Scanning Jalil JALALI 1, Maximilian EDER 2, Stefan RAITH 2, Alexander VOLF 2, Fee von WALDENFELS 2, Laszlo KOVACS
Breast Reconstruction Using Patients Own Tissue Based on CT Angiography and 3-D Surface Scanning Jalil JALALI 1, Maximilian EDER 2, Stefan RAITH 2, Alexander VOLF 2, Fee von WALDENFELS 2, Laszlo KOVACS
Title. CitationPhysica Medica, 30(5): Issue Date Doc URL. Type. File Information.
: Issue Date Doc URL. Type. File Information.") Title Preliminary analysis for integration of spot-scannin Author(s)Shimizu, S.; Matsuura, T.; Umezawa, M.; Hiramoto, K. CitationPhysica Medica, 30(5): 555-558 Issue Date 2014-07 Doc URL http://hdl.handle.net/2115/56596
Title Preliminary analysis for integration of spot-scannin Author(s)Shimizu, S.; Matsuura, T.; Umezawa, M.; Hiramoto, K. CitationPhysica Medica, 30(5): 555-558 Issue Date 2014-07 Doc URL http://hdl.handle.net/2115/56596
EVOLUTION IN 4D TREATMENT
 EVOLUTION IN 4D TREATMENT SIMULATION PLAN TREATMENT Innovative 4D SIGRT Solution Recent advances in treatment planning and delivery systems have led to consistently achieving optimal results. And now with
EVOLUTION IN 4D TREATMENT SIMULATION PLAN TREATMENT Innovative 4D SIGRT Solution Recent advances in treatment planning and delivery systems have led to consistently achieving optimal results. And now with
The Role of In-Room kv X-Ray Imaging for Patient Setup and Target Localization (TG104)
") The Role of In-Room kv X-Ray Imaging for Patient Setup and Target Localization (TG104) John Wong (jwong35@jhmi.edu) David Jaffray (David.Jaffray@rmp.uhn.on.ca) Fang-Fang Yin (fangfang.yin@duke.edu) AAPM
The Role of In-Room kv X-Ray Imaging for Patient Setup and Target Localization (TG104) John Wong (jwong35@jhmi.edu) David Jaffray (David.Jaffray@rmp.uhn.on.ca) Fang-Fang Yin (fangfang.yin@duke.edu) AAPM
Benchmark & FAQ for NRG BR001: A Phase 1 Study of SBRT for the Treatment of Multiple Metastases
 Benchmark & FAQ for NRG BR001: A Phase 1 Study of SBRT for the Treatment of Multiple Metastases Credentialing Requirements (SECTION 5) Facility Questionnaire Benchmark planning 3DCRT credentialing IMRT
Benchmark & FAQ for NRG BR001: A Phase 1 Study of SBRT for the Treatment of Multiple Metastases Credentialing Requirements (SECTION 5) Facility Questionnaire Benchmark planning 3DCRT credentialing IMRT