Mesenchymal Stem Cell Characterization. Peiman Hematti, M.D. Department of Medicine
|
|
|
- Reynold Copeland
- 5 years ago
- Views:
Transcription



1 Mesenchymal Stem Cell Characterization Peiman Hematti, M.D. Department of Medicine
")




2 Terminology has evolved over the years: Colony forming units-fibroblasts (CFU-E) Fibroblast colony forming cells (FCFC) Mesodermal progenitor cells Marrow stromal cells Multipotent marrow stromal cells Mesenchymal stem cells Terminology coined by Caplan in 1980 s due to their multilineage differentiation potential (bone, fat, cartilage, ) Mesenchymal stromal cells Mesnechymal stromal/stem cells CD105 CD73






3 Current view of MSCs JCI Tong Yin, et al. 116:1195 May 2006 Derivation of MSCs from Bone Marrow Basic Research Clinical Applications



4 The first report on clinical use of ex vivo culture expanded MSCs



5 The first report on use of allogeneic MSCs for nonhematological disorders MSC Plasticity


6


7 Figure 1 Immunomodulatory effects of MSCs Nauta, A. J. et al. Blood 2007;110: Copyright 2007 American Society of Hematology. Copyright restrictions may apply.


8 Promising results but most studies are small and nonrandomized Clinical Trials of MSCs Enhancement of HSC engraftment Autologous, Allogeneic HSCT Ex vivo expansion of cord blood CD34+ cells Treatment of congenital disorders Osteogenesis Imperfecta Metachromatic leukodystrophy, Hurler syndrome Immune modulation Graft versus host disease Prevention/treatment of rejection after solid organ transplant Autoimmune disorders (lupus, systemic sclerosis) Tissue regeneration Heart repair Acute myocardial infarction, chronic ischemia, heart failure COPD Crohn s disease Neurological disorders Amyotrophic lateral sclerosis, stroke, spinal cord injury, multiple sclerosis Diabetes Cirrhosis Acute kidney Injury Lower extremity ischemia Tissue repair after HSCT (perforated colon, pneumothorax, hemorrhagic cystitis) Tissue reconstruction Wound repair, fistula repair, soft tissue reconstruction Tracheal repair

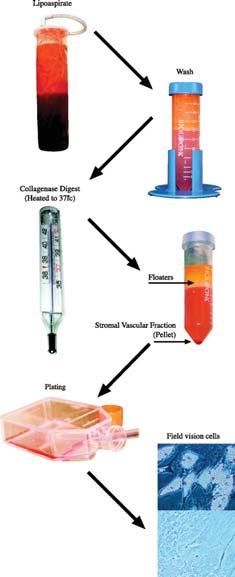


9 Adipose tissue-derived MSCs Gimble, J. M. et al. Circ Res 2007;100:


10 Bone Marrow Adipose Tissue Placenta Umbilical cord Muscle Heart Lung Pancreas Liver Kidney Bladder Tooth Synovia Ligament GI Tract
11 Factors to consider in use of MSC as a cell product Clinical indication State of disease to be used (early or late) Intended clinical effect Immune modulatory/paracrine effects/tissue replacement Cell dose and frequency of administration Route of administration Concomitant medications/treatments Staring tissue material: BM vs. fat, Autologous vs. allogeneic Culture methodology Plating density Passaging procedure (timing, plating density, ) Culture media FBS vs. platelet lysate vs. serum free media Passage of cells to be used Challenges in MSC Characterization No single marker exist for MSCs Current markers do not predict state of the cellular product or its capabilities Heterogeneous nature of cultured cells Poor understanding of how cells interact with other cells in vivo Poor understanding of how cells actually work in vivo Poor understanding of cell fate and survival post transplantation



12 Variables in MSC Production Preparation: Ficoll RBC lysis No prep Name: P0 or P1 First wash hours Seeding: 5,000/cm2-5,000,000/cm2 Variables in MSC Production Base medium: DMEM: Low Glucose High Glucose IMDM Alpha-MEM Serum: Heat inactivated or not Concentration % Platelet lysate Serum Free Culture additions: Antibiotics or no antibiotics FGF or other growth factors Other culture variables: Use of coated plates Hypoxia
13 Variables in MSC Production Passaging: % Confluency Time to passage: 7-28 days Frequency of media change Trypsinization method Passaging density Freezing method There is no standard culture methodology for MSCs MCT Culture method BM volume: 25 ml (fresh or frozen) MNC prep: Ficoll Medium: -MEM, 16.5% FBS, 1% GlutaMax Medium changes, frequency: days 1 and 2 to wash out non-adherent cells; then every 2-4 days Passes, length of culture: after 70-80% confluence at day 7-10, cells are inoculated into a cell factory at cells/cm2. On day at 70-80% confluence, cells are harvested for final prep Characterization: Flow cytometry: Positive for: CD73, CD90, CD105; Negative for : CD14, CD19, CD34, CD45, HLA-DR Functional/Potency Assays: Trilineage: Yes Suppression (NLR, CFSE, cytokines): Yes (limited) Other cytokines: N/A CFU: Initially attempted, but abandoned CHCT Culture method BM volume: 10 ml MNC prep: None, direct plating of whole BM Medium: -MEM, 10%FBS, 5ng/ml bfgf Medium changes, frequency: initially every 2-3 day to wash out non-adherent cells none once subculture Passes, length of culture: initial culture lasts about days, then we passage every 5-7 days Characterization: Flow cytometry: Positive for: CD90, CD73, CD29, CD105, CD166, HLA-ABC, Negative for : CD34, CD45, CD31 Functional/Potency Assays: Trilineage: only to validate the protocol originally Suppression (NLR, CFSE, cytokines): N/A Other cytokines: N/A CFU: N/A Other: depends on the project; the potency assay is specific/adapted to the function of the product CAGT Culture method BM volume: 25 ml fresh MNC prep: None- whole BM in Quantum Medium: DMEM, 5% human platelet lysate, Heparin, N- acetylcysteine, 1% GlutaMax Medium changes, frequency: wash out, day 3-4. Feed continuously (starting at 0.1 ml/min) doubling feed rate when lactate level >4.0 mm. Passes, length of culture: When lactate >4 mm and feeding at 1.6 ml/min, cells harvested. After P1, cells harvested when lactate >8 mm while feeding at 1.6 ml/min. Characterization: Flow cytometry: Positive for: CD73, CD90, CD105; Negative for : CD14, CD19, CD34, CD45, HLA-DR Functional/Potency Assays: Trilineage: Yes Suppression: No Other cytokines: N/A CFU: Yes



14 Characterization of MSC product Morphology Proliferation rate FACS per ISCT standards Differentiation assay (Bone, fat, cartilage formation) Functional in vitro assay: Differentiation Immunomodulatory Cytokine expression Gene expression Generation of MSCs: UW-PACT Effect of culture media on MSC morphology FBS StemPro MesenCult
15 Effect of culture media on MSC surface markers FBS IRRAD P2 FBS IRRAD P5 FBS NONIRRAD P2 FBS NONIRRAD P5 MESENCULT P2 MESENCULT P5 StemPro P2 StemPro P5 MFI CD105 MFI CD73 MFI CLASS I MFI CD90 Cell surface markers can not differentiated between different MSC products Goals of Potency Assay Development To develop assays for comparison of functional properties of MSCs generated with different culture methodologies Easy to perform, Reproducible and Comprehensive, if possible Identify a potency assay that is predictive of efficacy outcome (FDA expectation to be developed by phase-iii trials) Potency assay for different clinical indications?


16 PACT Immunopotency Assay: Inhibition of CD4+ T cell Proliferation CFSE-label PBMCs to track proliferation. MSCs added at titrated ratios. Anti-CD3 and anti-cd28 used in 4 day T cell stimulation. Needs cell/cell contact. CD4 1-0 PBMC:MSC 1-1 PBMC:MSC PBMC:MSC CFSE Reproducibility of Immunopotency Assay 3 Different Assays on 3 Different Days
17 Application of the Immunopotency Assay Reference Std MSCs with LPK1 Reference Std MSCs with LPK % Proliferation (cfse-lo) STEM PRO P2 FBS P2 % Proliferation (cfse-lo) STEM PRO P2 FBS P P-M 1-0 P-M 1-1 P-M P-M P-M P-M 1-0 P-M 1-1 P-M P-M P-M PBL-MSC Ratio PBL-MSC Ratio Determine potency of MSCs grown in various types of media FBS consistently outperforms StemPro (both at the P2 and P5) sil-2r Levels in the supernatants correlates with T cell proliferation suppression Correlation Between the Two Assays: R 2 ~1.0
18 Factors to consider in use of MSC as a cell product Staring source Autologous vs. allogeneic BM versus fat versus other tissues Production methodology Starting material processing, plating density, passaging procedure Culture media (FBS vs. platelet lysate vs. serum free media) Characterization Lack of markers for identification of cell state Lack of comprehensive potency assay Poor understanding of cell fate and function in vivo Lack of correlation between in vitro assays, in vivo animal models and clinical results Clinical indication State of disease to be used (early or late) Route of administration, Cell dose and frequency Concomitant medications/treatments Intended clinical effect Immune modulatory Paracrine effects Tissue replacement Thanks