The Newcastle Upon Tyne Hospitals NHS Foundation Trust. Clinical Practice Guidelines & Protocols Policy
|
|
|
- Jocelin Watts
- 5 years ago
- Views:
Transcription
1 The Newcastle Upon Tyne Hospitals NHS Foundation Trust Clinical Practice Guidelines & Protocols Policy Version No.: 4.4 Effective From: 23 February 2017 Expiry Date: 23 February 2020 Date Ratified: 23 February 2017 Ratified By: Clinical Effectiveness, Audit and Guidelines Committee 1 Introduction This policy covers the standards and methods to be used in the development, ratification, review and dissemination of Clinical Practice Guidelines and Protocols within The Newcastle upon Tyne Hospitals NHS Foundation Trust. Clinical Practice Guidelines and Protocols should be in place in all Clinical Specialties for the most commonly used procedures. 2 Scope This policy applies to all members of staff working within The Newcastle upon Tyne Hospitals NHS Foundation Trust who are involved in any aspect of developing or reviewing clinical guidelines and protocols. This document scope covers the development, approval and presentation of guidelines and protocols as defined in paragraph 5. This policy does not cover principles to be applied to the development of Trust policies and procedures, which are covered under the Policies and Procedural Documents: Development, Approval and Dissemination Policy. 3 Aim of the policy The aim of this policy is to ensure an up to date, evidence-based set of Clinical Practice Guidelines and Protocols underpinning health care for patients of The Newcastle upon Tyne Hospitals NHS Foundation Trust. This aim will be achieved by means of: rigorous methods used in the development and ratification of evidencebased Clinical Practice Guidelines and Protocols process of endorsement of externally produced guidelines for use within the Trust processes to identify duplications and/or gaps in the set of Clinical Practice Guidelines and Protocols and to address those duplications/gaps a review process carried out on a regular basis using a common standard for appraisal version control and archiving arrangements Clinical Audit driven by Clinical Practice Guidelines and Protocols. Page 1 of 19
2 4 Duties Roles and Responsibilities 4.1 Clinical Governance and Quality Committee The Clinical Governance and Quality Committee has ultimate responsibility for ensuring effective, evidence-based practice is promoted within the Trust underpinned by robust clinical guidelines and protocols. 4.2 Clinical Effectiveness, Audit and Guidelines Committee The Clinical Effectiveness, Audit and Guidelines Committee has delegated responsibility for ensuring effective, evidence-based practice is promoted within the Trust, by monitoring the processes for developing, reviewing and archiving clinical guidelines and protocols 4.3 Clinical Governance and Risk Department (CGARD) CGARD has delegated responsibility for ensuring an effective, robust system is in place for the review and publication of all clinical guidelines and protocols within the Trust. CGARD also has responsibility for the archiving of guidelines and protocol documents within the organisation. The Clinical Effectiveness Manager within the Department has overall responsibility for the content of the clinical guidelines database on the Intranet. This includes the ongoing development, management and administration of the database. 4.4 Trust Committees Trust Committees with responsibility for clinical practice are responsible for carrying out the approval of guidelines and protocols that fall within their remit, according to the processes outlined in this policy. 4.5 Clinical Directors Clinical Directors are responsible for ensuring that there is a robust system in place within their Directorate for the approval of guidelines and protocols that fall entirely within their remit, according to the processes outlined in this policy, although the actual processes may be delegated to appropriate specialists / professions within the Directorate, or to the Directorate Clinical Governance Lead. 4.6 Guideline/Protocol Authors The author retains ownership through development, consultation, approval and ratification processes. Responsibility for monitoring and review of the guideline/protocol remains with the author after release of the final version to the Clinical Effectiveness Manager, CGARD. Page 2 of 19
3 The author of the guideline/protocol must check that the proposed new guideline subject is not already covered by an existing policy document or guideline, or could not easily be incorporated into an existing policy document or guideline. The author of the guideline/protocol must ensure that the guideline/protocol is written in the agreed Trust format (see Appendix 1). The author must ensure that appropriate consultation with expert individuals or groups must take place, to ensure accuracy and adherence with existing Trust procedures and current evidence based practice. When notified that a guideline/protocol for which they are responsible is approaching or past its review deadline, it is the responsibility of the author to instigate a review process and update the guideline/protocol as necessary. 4.7 Wards and Departments It is the responsibility of all wards and departments to make staff aware that new or amended guidelines and protocols relevant to their area are available in response to the update notification from CGARD. Paper copies of Trust guidelines and protocols are discouraged, but if wards and departments do keep such copies there must be systems in place to keep these updated and it must be acknowledged that the definitive version is that displayed on the Intranet site. All new staff should be made aware of how to find and use Trust relevant guidelines during their induction programme as outlined in the Induction Policy. 4.8 All Staff All staff within The Newcastle upon Tyne Hospitals NHS Foundation Trust are responsible for ensuring that the principles outlined within this policy are universally applied and that they familiarise themselves with all guidelines and protocols relevant to their area of work. 5 Definitions 5.1 Policy A policy enables management and staff to make correct decisions; deal effectively with and comply with relevant legislation, regulations, organisational rules and good practice. A policy document should be regarded as mandatory, with deviation only in exceptional circumstances, as it sets out a course of action which the Trust expects to be followed. Trust policies have been formulated and developed to guide staff in their Page 3 of 19
4 5.2 Procedure work ensuring their protection and that of service users, in order to minimise risk and maximise safety for all concerned. A set of detailed step by step instructions that describe the appropriate method for carrying out tasks or activities to achieve the highest standards possible and to ensure efficiency, consistency and safety. 5.3 Protocols Protocols are rigid statements allowing little or no flexibility or variation. A protocol sets out a precise sequence of activities to be adhered to in the management of a specific clinical condition. 5.4 Guidelines Clinical guidelines are systemically developed statements that assist clinicians and patients in making decisions about appropriate treatments for specific conditions. They allow deviation from a prescribed pathway according to the individual circumstances and where reasons can be clearly demonstrated and documented. Endorsed guidelines are, by definition, those which practitioners are encouraged to follow. 6 The Development and Ratification of Clinical Guidelines and Protocols 6.1 Development of local guidelines and protocols The development of guidelines and protocols by Trust staff for use across the Trust and/or specified Directorates needs to be undertaken following a process which ensures that the guidance is of a high standard and evidence based. The development and ratification of new internal guidelines and protocols must follow the procedures set out in Appendix 2 and guidelines must be written in the format and containing the minimum content as at Appendix 1. This involves a process of review by the appropriate specialists within the Trust and final ratification by the Clinical Director (or their nominated delegate), Lead Clinician or Chairman of the appropriate committee. 6.2 Review of local guidelines and protocols When an internally produced guideline/protocol is due to be reviewed, to ensure that it still contains an accurate evidence base, the processes outlined in Appendix 3 should be followed. When the guideline/protocol has completed the review process, it will be displayed on the intranet with the date reflecting any recent review of content and the current status of the document. Page 4 of 19
5 As each existing internal guideline/protocol comes up for review it is appraised and revised accordingly, if necessary, starting with the formation of a multi-disciplinary team and a literature search and again requiring final ratification by the appropriate Clinical Director (or their nominated delegate), Lead Clinician or Chairman of the appropriate committee. 6.3 Endorsement of new External Guidelines and Protocols Guidelines and protocols which are published by bodies including NICE and professional colleges also need to ratified by Trust clinicians to ensure that they are clinically effective and safe for use within our organisation. Externally produced guidelines undergo a process of endorsement which is outlined in Appendix Publication of Clinical Practice Guidelines and Protocols Both internally and externally produced guidelines and protocols which have been ratified for use within the Trust are displayed on the Clinical Guidelines database on the intranet and available to staff. The intranet display includes the date of publication and whether it is an internally or externally produced document which is endorsed for use or for reference only. Trust Policies are held on the Trust Policies database and Clinical Practice Guidelines and Protocols on the Clinical Guidelines database. Revisions to the Clinical Guidelines Database are published quarterly in a Newsletter to all Clinical Directorates; the Newsletter is also placed on the Intranet. Clinical Practice Guidelines and Protocols developed locally and held on the Clinical Guidelines database are covered by the Freedom of Information Act (2000). 6.5 Control of Clinical Guidelines and Archiving The Clinical Guidelines database follows the precedent set by the Trust Policies database in that the Intranet version, rather than the paper document, is the definitive version of an internal guideline/protocol document and this version should therefore be used in clinical practice. Each guideline should contain the effective from date and review date to ensure that the latest version is published and this will be held on the database for each guideline. The Clinical Guidelines database also holds an archive of all guidelines/protocols produced internally. As each guideline/protocol is superseded the previous version is archived within the guidelines database and can therefore be retrieved for reference as required. In order to ensure that internal guidelines are up to date the standard review Page 5 of 19
6 period will be between one and three years, any internal guideline more than 6 months past its review date may be archived off the database; it can of course be reinstated if and when the review process is completed. The Clinical Effectiveness Manager will make sure that copies of earlier versions of all guidelines and protocols are archived and subsequently deleted in line with the Corporate Records Policy. 6.6 Annual Review Directorates are responsible for the annual review of their guidelines/protocols to identify gaps, inconsistencies and duplications. Monitoring and review of this process is undertaken by the Clinical Effectiveness, Audit and Guidelines Committee (CEAGC) and each Audit Lead will report annually to this group on the effectiveness of the process within their Directorate. Guidelines which affect multiple Directorates need to be reviewed by the relevant committee(s). 6.7 Clinical Audit Compliance with endorsed guidelines is determined by the Clinical Audit of guidelines and procedures. Each Directorate draws up an annual plan showing the audits to be carried out and their priority, incorporating any applicable national audits, in accordance with the Trust s Clinical Audit Policy. 7 Training Appropriate staff within CGARD will be trained on this policy and the management of the Clinical Guidelines database. An on-line training package is available on the intranet in the use of the guidelines/protocols intranet site, and number of resources are also available on the development, appraisal and implementation of clinical guidance. No other formal training is required in relation to the policy. Staff are advised to contact the Clinical Effectiveness Manager for advice in relation to guideline / protocol development. 8 Equality and diversity The Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds. This policy has been appropriately assessed. 9 Monitoring the compliance/effectiveness of this policy Monitoring compliance with this policy will be the responsibility of the Clinical Effectiveness Manager. This will be undertaken by: Page 6 of 19
7 Standard / process issue Compliance with Trust guidelines format including: Compliance with; Style and format Structure Compliance with review process Compliance with the requirement to have robust systems in place within Directorates for the development and review of clinical guidelines Compliance with requirement to complete Review Forms for all new and revised guidelines and protocols Compliance with the requirement to archive old versions of guidelines and protocols Monitoring and audit Method By Committee Frequency Assessing all The Clinical CEAGC Ongoing new and Effectiveness reviewed Manager guidelines against the agreed format before updating the guidelines database Monitoring of database with preparation of a status report on guideline reviews Included in Annual Audit Report Audit of new and revised guidelines and protocols during the year Audit of archived files The Clinical Effectiveness Manager Directorate Clinical Audit Leads The Clinical Effectiveness Manager The Clinical Effectiveness Manager CEAGC CEAGC CEAGC CEAGC Quarterly Annual Annual Annual 10 Consultation and review of this policy This policy has been reviewed in consultation with the Clinical Effectiveness Manager, the Quality and Clinical Effectiveness Manager, and the Director of Quality and Clinical Effectiveness. This policy will be reviewed every three years by the Clinical Effectiveness, Audit and Guidelines Committee (CEAGC). Any comments are to be addressed to the Information Systems Analyst Page 7 of 19
8 11 Implementation of policy (including raising awareness) This policy will be publicised by the Clinical Effectiveness Manager in the Trust Policy Newsletter and published on the Trust Intranet. All guidelines will be reviewed in light of this policy and rewritten, where required, to conform to the layout and content requirements stipulated. 12 References 1. Freedom of Information Act London: Stationery Office. Available at 13 Associated documentation This policy relates to all clinical guidelines and protocols within the organisation. See also the: Clinical Audit Policy Implementation of NICE Guidelines Policy Corporate Records Policy Policies and Procedural Documents: Development, Approval and Dissemination Policy Page 8 of 19
9 Appendix 1 Format of Guideline Documents The guideline should be produced in a clear, accessible format (which accommodates the need for viewing electronically as well as from hard copy); local Guidelines should follow the layout format as set out below. The Newcastle upon Tyne Hospitals NHS Foundation Trust Guideline Title Version No.: Effective From: Full date (e.g. 1 July 2014) Expiry Date: Full date (e.g. 1 July 2014) Date Ratified: Full date (e.g. 1 July 2014) Ratified By: Owning Trust Committee/Clinical Director/Lead Clinician 1 Introduction 2 Guideline scope For example. which patient cohort this does (or does not) apply to, the audience for whom it is intended. 3 Main Body of the guideline 4 Training, Implementation, Resource Implications 5 Monitoring Section This should include what will be monitored, i.e. the content of the audit, who will gather this information, which group it will be presented to and the frequency at which this will occur, e.g. The organisation continually strives to achieve 100% compliance with this guideline and its intended outcomes. Where this is not met an action plan will be formulated and reviewed until completion. Please see the table below for standards and monitoring arrangements: Page 9 of 19
10 Standards This should be the steps that you have described in the process part of the guideline for example: Monitoring and audit Method By Group / This is how are you going to monitor this, for example: Snapshot random audit Who will undertake the monitoring: Infant feeding lead Committee Who has overall accountability: CGQ Frequency How often are these carried out: at least monthly quarterly All inpatients will receive an initial NEWS score within an hour of admission Once you have pulled all the standards out of the guideline you then need to put in your outcome standards, for example: Reduction in the rate of unexpected cardiac arrests Quality assurance audit Outcomes may be monitored differently for example: Review of all incidents of unexpecte d cardiac arrests Review of rates and reasons of cardiac arrests As above As above If this is a review of incidents or complaints etc it should be continuous Continuously Annually The audit tool should be included as an appendix to the guideline. 6 Evidence Review and Evaluation 7 References All guidelines must consider any new or revised external reports or guidance and reference must be made to NICE guidance in particular where this is applicable. Page 10 of 19
11 Appendix 1.2 Protocol Minimum Data Set Local Protocols do not have a prescribed layout but should contain the minimum dataset of: title, scope and purpose (i.e. the overall aim of the guidance, the specific clinical questions and the target population), evidence base, references and recommendations, (it is acknowledged that in some circumstances there may be no evidence base for Protocols), authorship / membership of the development group, date of publication and review date, points for audit, and in addition they may include, points for further research/discussion, development method employed (including literature search), resource requirements. Page 11 of 19
12 Appendix 1.3 General Principles for Writing Guidelines/Protocols 1. Guidelines are to be produced to a standard format as outlined in Appendix The intended audience should be targeted and it should be ensured that anyone who reads the document will be able to understand it. 3. The information should be presented in a logical, sequential order. 4. The content of each guideline/protocol should comply with all relevant legal and statutory requirements, NHS guidance and policy in force at the time of writing or review and should reflect evidence based best practice. 5. Consider what relevant guideline/protocols documents already exist in the Trust and cross-reference where appropriate to avoid duplication. 6. A summary or introduction at the beginning of each guideline/protocol outlining the aims of the guideline/protocol and its application should be included. 7. The possibility of patient groups being involved in the production of policy/procedure should be considered. 8. Ensure that what is proposed does not make it impossible or unreasonably difficult for people to make use of any service that is being proposed or provided due to their age, gender, disability, language or race. The needs of people from diverse cultural or religious groups and general health and safety issues are to be considered. 9. Be aware that under the Freedom of Information Act there may be open access to your document by the general public. 10. Be aware that the guideline/protocol document will be viewed electronically and good practice to view in this format is: Do not have a series of cover pages, contents lists and/or blank pages at the beginning of the document, which takes a while to load up and click past before the user gets the heart of the documents message. Include appropriate references, acknowledgements and any appendices at the end of the document. All Trust guidelines/protocols should: be written in Arial 12; be justified to the left; include page numbers in the footer of the document in the format Page x of y; use plain English with explanations of acronyms (go to for a guide to plain English); use flow diagrams where possible; and Page 12 of 19
13 avoid the use of block capitals. Block capitals make the text difficult to read because the shapes of words disappear, causing the reader to slow down and study each letter. Ironically, readers tend to skip sentences written in all uppercase. To highlight information and maintain readability, use bold or italic text. Avoid underling text for emphasis (in online documents underlining implies a hypertext link) Hypertext links should be underlined and in blue Capital letters should be used for referring to formal or specific committees, e.g. Patient, Quality, Risk and Safety Committee. This also applies to the title of individuals, e.g. Director of Finance and Information. Lower case letters should be used for generic reference, e.g. divisional managers, executive directors. Page 13 of 19
14 Appendix 2 Procedure for Developing Internal Guidelines and Protocols The following methodology is to be used for the development of new internal guidelines: a check is carried out that appropriate organisations are not in the process of developing such a guideline; a multidisciplinary team (MDT) is set up with clearly delineated scope and responsibilities, incorporating representation from patients where necessary; a comprehensive literature search is carried out (involving a librarian if necessary); the guideline is evaluated by a peer review group, in a small minority of situations, an external peer review may be appropriate; the guideline is generally piloted before final approval and general dissemination; dissemination of the guideline should include a plan for implementation, including specific training requirements, resource requirements and timescales. following the process of peer review by the appropriate specialist(s) and interested bodies, the final approval sign off should be by the Clinical Director or his/her nominee. New resources Where guidelines require new resources the guideline will need to be referred to the appropriate body with sufficient authority to sanction the new resources. Page 14 of 19

15 Procedure for Developing Internal Guidelines and Protocols Page 15 of 19
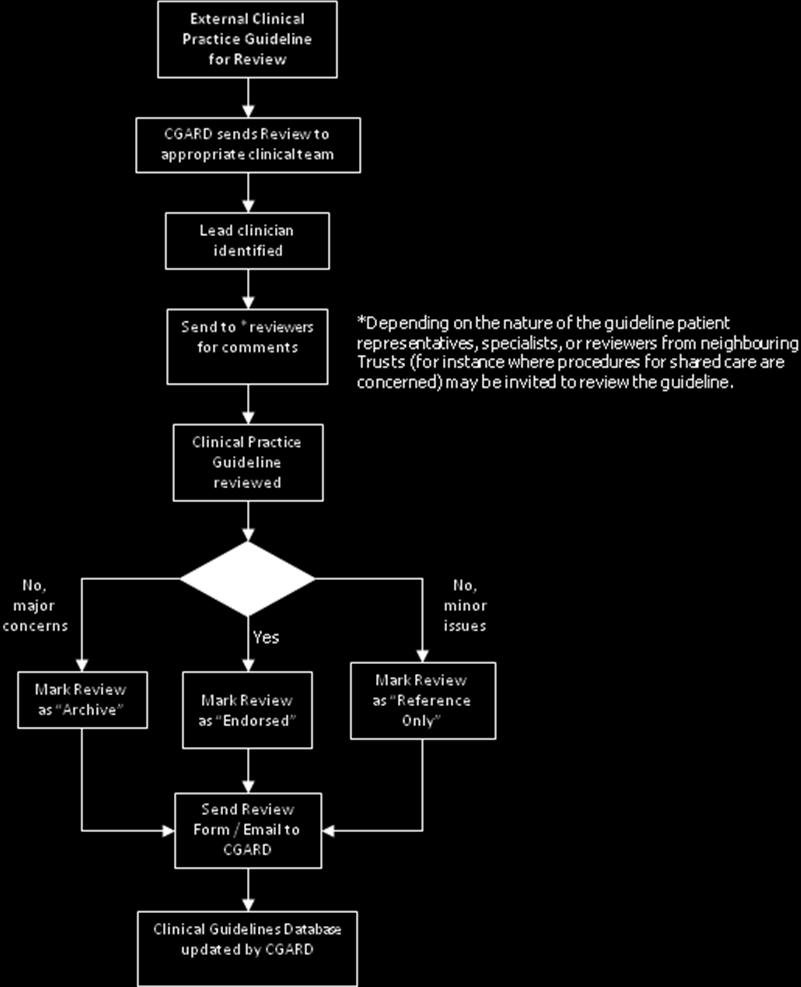
16 Procedure for the Review of Internal Guidelines Appendix 3 The normal path for review and endorsement of Clinical Practice Guidelines is via a multi-disciplinary Review Team within each Directorate. This consists of a process of peer review by the appropriate specialist(s) and interested bodies, with final sign off by the Clinical Director or his/her nominee (see flow diagram below). Where a guideline is to be used for shared care with another NHS Trust then the appropriate representative(s) from that Trust should be included in the review process. Likewise, where there are areas that involve patients (e.g. discussion of visitors facilities) then patient and visitor representatives should be consulted. Two to three months before the review date falls due the Clinical Governance and Risk Department (CGARD) sends an Internal Clinical Guidelines Review Form to the relevant Directorate requesting review of the guideline. The Directorate decides whether any specialists or external personnel need to be involved in the review, depending on the nature of the guideline. One person is designated as the lead to oversee the review process. The guideline is amended where necessary in the light of recent research, to reflect changes in local practice, learning from experience and changes in fine detail, e.g. changes to contact details. The guideline is then be circulated to the reviewers, if the guideline is accepted by the reviewers the review form is completed accordingly including the future review date and returned to CGARD, together with the revised guideline, to update the database. If the reviewers require further changes, the guideline is amended and re-submitted for review until accepted. On occasion a guideline may be considered too out of date or redundant and CGARD will be asked to archive the guideline off the database. (Archived guidelines can still be accessed by CGARD). If the results of a review are not returned within two months a reminder is sent out by the CGARD and further reminders every month thereafter. The normal path for review and endorsement of Clinical Practice Guidelines that fall outside the remit of an individual Directorate and apply to a service crossing many Directorates, e.g. Critical Care, is via a multi-disciplinary Review Team across multiple Directorates incorporating peer review by the appropriate specialists and interested bodies, with final sign off by the lead clinician for that speciality, e.g. Chair of Critical Care Executive or the Clinical Director. Where guidelines need to be reviewed by standing Committees, e.g. Medicines Management Committee, etc., the groups involved should be authorised by the Clinical Governance and Quality Committee to review and endorse Clinical Practice Guidelines. Expiry of internal guidelines In order to ensure that internal guidelines are up to date the standard review period will be between one and three years, any internal guideline more than 6 months past its review date may be archived off the database; it can of course be reinstated if and when the review process is completed. Page 16 of 19
17 Procedure for Review of Internal Guidelines Internal Clinical Practice Guideline due for Review CGARD sends Review request to Reviewer Reviewer carries out analysis of evidence and current practice Content of guideline revised (if necessary) & sent for comment* *Depending on the nature of the guideline patient representatives, specialists, or reviewers from neighbouring hospitals (for instance where procedures for shared care are concerned) may be invited to review the guideline. No, minor concerns Clinical Practice Guideline reviewed Accepted? Yes Next review date agreed Mark Review as Archive No, major concerns Clinical Practice Guideline published and sent with Review Form to CGARD Clinical Guidelines Database updated by CGARD Page 17 of 19
18 Appendix 4 Procedure for the Endorsement of External Guidelines Process External guidelines are generally only reviewed as they are received in the Trust, to determine whether or not they are endorsed for use within the Trust. A guideline can either be endorsed, left as for reference only, or be archived off the database. The funding of Technology Appraisal Guidelines (TAGs) developed by the National Institute for Health and Care Excellence (NICE) is mandatory for all NHS Trusts within three months of publication; therefore, the review of TAGs should be completed within three months of publication (see NICE Guidelines Implementation Policy) If a guideline is endorsed but some local variation in implementation needs to be documented this would necessitate the drawing up of an internal guideline to be linked to the external guideline on the database. New resources Where guidelines require new resources the guideline will need to be referred to the appropriate body with sufficient authority to sanction the new resources. Page 18 of 19

19 Page 19 of 19
20 The Newcastle upon Tyne Hospitals NHS Foundation Trust Equality Analysis Form A This form must be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval. PART 1 1. Assessment Date: 12/02/ Name of policy / strategy / service: Clinical Practice Guidelines & Protocols Policy 3. Name and designation of Author: Bernadette Risebury 4. Names & designations of those involved in the impact analysis screening process: Bernadette Risebury, Information Systems Analyst 5. Is this a: Policy x Strategy Service Is this: New Revised x Who is affected Employees x Service Users Wider Community 6. What are the main aims, objectives of the policy, strategy, or service and the intended outcomes? (These can be cut and pasted from your policy) This policy covers the standards and methods to be used in the development, ratification, review and dissemination of Clinical Practice Guidelines and Protocols within The Newcastle upon Tyne Hospitals NHS Foundation Trust. Clinical Practice Guidelines and Protocols should be in place in all Clinical Specialties for the most commonly used procedures 7. Does this policy, strategy, or service have any equality implications? Yes No x If No, state reasons and the information used to make this decision, please refer to paragraph 2.3 of the Equality Analysis Guidance before providing reasons:
21 8. Summary of evidence related to protected characteristics Protected Characteristic Race / Ethnic origin (including gypsies and travellers) Evidence, i.e. What evidence do you have that the Trust is meeting the needs of people in various protected Groups The policy asks for all guideline authors to involve relevant patient groups wherever applicable/appropriate when developing and reviewing guidelines Does evidence/engagement highlight areas of direct or indirect discrimination? If yes describe steps to be taken to address (by whom, completion date and review date) Sex (male/ female) As above As above Religion and Belief As above As above Sexual orientation including As above As above lesbian, gay and bisexual people Age As above As above Disability learning difficulties, physical disability, sensory impairment and mental health. Consider the needs of carers in this section As above As above Gender Re-assignment As above As above Marriage and Civil Partnership As above As above Maternity / Pregnancy As above As above 9. Are there any gaps in the evidence outlined above? If yes how will these be rectified? No Does the evidence highlight any areas to advance opportunities or foster good relations. If yes what steps will be taken? (by whom, completion date and review date) This policy relates to clinical procedures 10. Engagement has taken place with people who have protected characteristics and will continue through the Equality Delivery System and the Equality Diversity and Human Rights Group. Please note you may require further engagement in respect of any significant changes to policies, new developments and or changes to service delivery. In such circumstances please contact the Equality and Diversity Lead or the Involvement and Equalities Officer. Do you require further engagement? Yes No x 11. Could the policy, strategy or service have a negative impact on human rights? (E.g. the right to respect for private and family life, the right to a fair hearing and the right to education? No
22 PART 2 Name: Bernadette Risebury Date of completion: 12/02/2017 (If any reader of this procedural document identifies a potential discriminatory impact that has not been identified, please refer to the Policy Author identified above, together with any suggestions for action required to avoid/reduce the impact.)
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Sustainability Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Sustainability Policy Version No.: 2.0 Effective From: 22 December 2017 Expiry Date: 22 December 2020 Date Ratified: 20 July 2017 Ratified By: Sustainable
The Newcastle upon Tyne Hospitals NHS Foundation Trust Sustainability Policy Version No.: 2.0 Effective From: 22 December 2017 Expiry Date: 22 December 2020 Date Ratified: 20 July 2017 Ratified By: Sustainable
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Energy Policy
 1 Introduction The Newcastle upon Tyne Hospitals NHS Foundation Trust Policy Version No.: 4 Effective From: 05 July 2017 Expiry Date: 05 July 2020 Date Ratified: 30 May 2017 Ratified By: Sustainable Healthcare
1 Introduction The Newcastle upon Tyne Hospitals NHS Foundation Trust Policy Version No.: 4 Effective From: 05 July 2017 Expiry Date: 05 July 2020 Date Ratified: 30 May 2017 Ratified By: Sustainable Healthcare
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Sustainable Procurement Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Sustainable Procurement Policy Version No.: 1.1 Effective From: 14 April 2016 Expiry Date: 14 April 2019 Date Ratified: 1 March 2016 Ratified By:
The Newcastle upon Tyne Hospitals NHS Foundation Trust Sustainable Procurement Policy Version No.: 1.1 Effective From: 14 April 2016 Expiry Date: 14 April 2019 Date Ratified: 1 March 2016 Ratified By:
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Employment Policies & Procedures
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies & Procedures Maintaining Services During Adverse Weather Conditions and Public Transport Disruption Policy Version.: 3.0 Effective
The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies & Procedures Maintaining Services During Adverse Weather Conditions and Public Transport Disruption Policy Version.: 3.0 Effective
POLICY MANAGEMENT FRAMEWORK
 POLICY MANAGEMENT FRAMEWORK October 2012 Author: Responsibility: Janet Young, Governance and Risk Manager All Staff Effective Date: ctober 2012 Review Date: October 2014 Reviewing/Endorsing committees
POLICY MANAGEMENT FRAMEWORK October 2012 Author: Responsibility: Janet Young, Governance and Risk Manager All Staff Effective Date: ctober 2012 Review Date: October 2014 Reviewing/Endorsing committees
POLICY ON MANAGING POLICIES, PROCEDURES AND GUIDANCE DOCUMENTS
 POLICY ON MANAGING POLICIES, PROCEDURES AND GUIDANCE DOCUMENTS Version: 6 Date Ratified: February 2017 Review Date: February 2020 Applies to: Senior Managers and staff who produce procedural documents.
POLICY ON MANAGING POLICIES, PROCEDURES AND GUIDANCE DOCUMENTS Version: 6 Date Ratified: February 2017 Review Date: February 2020 Applies to: Senior Managers and staff who produce procedural documents.
The Newcastle upon Tyne Hospitals Foundation NHS Trust. Employment Policies and Procedures
 The Newcastle upon Tyne Hospitals Foundation NHS Trust Employment Policies and Procedures Staff Leaving the Trust or Moving within the Trust Procedure Version No.: 5.6 Effective Date: 13 December 2017
The Newcastle upon Tyne Hospitals Foundation NHS Trust Employment Policies and Procedures Staff Leaving the Trust or Moving within the Trust Procedure Version No.: 5.6 Effective Date: 13 December 2017
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Volunteer Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Volunteer Policy Version No.: 2.1 Effective From: 23 December 2015 Expiry Date: 23 December 2018 Date Ratified: 2 December 2015 Ratified By: Employment
The Newcastle upon Tyne Hospitals NHS Foundation Trust Volunteer Policy Version No.: 2.1 Effective From: 23 December 2015 Expiry Date: 23 December 2018 Date Ratified: 2 December 2015 Ratified By: Employment
TRUST-WIDE NON-CLINICAL POLICY DOCUMENT. Date Ratified: February 2015 Next Review Date (by): Interim Review August 2017 Version Number: 2015 Version 1
: Interim Review August 2017 Version Number: 2015 Version 1") TRUST-WIDE NON-CLINICAL POLICY DOCUMENT Policy Number: Scope of this Document: Recommending Committee: Appproving Committee: SA01 All Staff Policy Group Executive Committee Date Ratified: February 2015
TRUST-WIDE NON-CLINICAL POLICY DOCUMENT Policy Number: Scope of this Document: Recommending Committee: Appproving Committee: SA01 All Staff Policy Group Executive Committee Date Ratified: February 2015
NORTH EAST HAMPSHIRE AND FARNHAM CLINICAL COMMISSIONING GROUP POLICY FOR THE MANAGEMENT OF POLICIES AND CORPORATE DOCUMENTS
 NORTH EAST HAMPSHIRE AND FARNHAM CLINICAL COMMISSIONING GROUP POLICY FOR THE MANAGEMENT OF POLICIES AND CORPORATE DOCUMENTS Document Control Sheet Version 1 Date 22 October 2013 Status Draft Author Justina
NORTH EAST HAMPSHIRE AND FARNHAM CLINICAL COMMISSIONING GROUP POLICY FOR THE MANAGEMENT OF POLICIES AND CORPORATE DOCUMENTS Document Control Sheet Version 1 Date 22 October 2013 Status Draft Author Justina
Development and Management of Procedural Documents Policy
 Development and Management of Procedural Documents Policy The 5 key messages the reader should note about this document are: 1. Procedural Documents are important within any organisation. They are an essential
Development and Management of Procedural Documents Policy The 5 key messages the reader should note about this document are: 1. Procedural Documents are important within any organisation. They are an essential
The Newcastle Upon Tyne Hospitals NHS Foundation Trust. Aggregating Data and Learning from Incidents, Complaints and Claims Policy
 The Newcastle Upon Tyne Hospitals NHS Foundation Trust Aggregating Data and Learning from Incidents, Complaints and Claims Policy Version no. 2.1 Effective from: 2 nd October 2012 Expiry date: 31 st October
The Newcastle Upon Tyne Hospitals NHS Foundation Trust Aggregating Data and Learning from Incidents, Complaints and Claims Policy Version no. 2.1 Effective from: 2 nd October 2012 Expiry date: 31 st October
This Policy supersedes the following Policy, which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Forensic Readiness Policy NTW(O)56 Lisa Quinn Executive Director of Performance and Assurance Sue Proud Information
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Forensic Readiness Policy NTW(O)56 Lisa Quinn Executive Director of Performance and Assurance Sue Proud Information
Performance Development Review (Appraisal) Policy
 Policy") Performance Development Review (Appraisal) Policy Executive Director lead Author / Lead Feedback on implementation to Dean Wilson, Director of Human Resources Jennie Wilson / Dean Wilson Jennie Wilson,
Performance Development Review (Appraisal) Policy Executive Director lead Author / Lead Feedback on implementation to Dean Wilson, Director of Human Resources Jennie Wilson / Dean Wilson Jennie Wilson,
This Policy supersedes the following Policy, which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Forensic Readiness Policy NTW(O)56 Lisa Quinn, Executive Director of Commissioning and Quality Assurance Angela
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Forensic Readiness Policy NTW(O)56 Lisa Quinn, Executive Director of Commissioning and Quality Assurance Angela
Freedom of Information (FOI) Policy
 Policy") Freedom of Information (FOI) Policy Subject Freedom of Information Act (2000) Policy number Tbc Approved by Trust Executive Group Date approved March 2015 Version 2 Policy owner Director of Communications
Freedom of Information (FOI) Policy Subject Freedom of Information Act (2000) Policy number Tbc Approved by Trust Executive Group Date approved March 2015 Version 2 Policy owner Director of Communications
Controlled Document Number: Version Number: 7 Controlled Document Sponsor: Controlled Document Lead:
 Policy for the Development and Management of Controlled Documents CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE: Controlled Document Number: Version Number: 7 Controlled Document Sponsor: Controlled
Policy for the Development and Management of Controlled Documents CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE: Controlled Document Number: Version Number: 7 Controlled Document Sponsor: Controlled
Royal National Hospital for Rheumatic Diseases NHS Foundation Trust. Equal Opportunities in Employment
 Royal National Hospital for Rheumatic Diseases NHS Foundation Trust T 01225 465941 F 01225 421202 E info@rnhrd.nhs.uk W www.rnhrd.nhs.uk Royal National Hospital for Rheumatic Diseases NHS Foundation Trust,
Royal National Hospital for Rheumatic Diseases NHS Foundation Trust T 01225 465941 F 01225 421202 E info@rnhrd.nhs.uk W www.rnhrd.nhs.uk Royal National Hospital for Rheumatic Diseases NHS Foundation Trust,
Secondary Employment Policy
 Secondary Employment Policy Controlled document This document is uncontrolled when downloaded or printed. Reference number Version 3 Author & Job Title Executive Lead WHHT: HR046 Christine Taylor, ER Team
Secondary Employment Policy Controlled document This document is uncontrolled when downloaded or printed. Reference number Version 3 Author & Job Title Executive Lead WHHT: HR046 Christine Taylor, ER Team
CCG CO12 Policy and Framework for Partnership Governance
 Corporate CCG CO12 Policy and Framework for Partnership Governance Version Number Date Issued Review Date V2: 21/02/2015 29/04/2015 21/02/2018 Prepared By: Consultation Process: Formally Approved: 25/02/2015
Corporate CCG CO12 Policy and Framework for Partnership Governance Version Number Date Issued Review Date V2: 21/02/2015 29/04/2015 21/02/2018 Prepared By: Consultation Process: Formally Approved: 25/02/2015
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Young Persons and Work Experience Students Under 18 Years of Age Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Young Persons and Work Experience Students Under 18 Years of Age Policy Version No: 4.2 Effective From: 4 April 2016 Expiry Date: 4 April 2019 Date
The Newcastle upon Tyne Hospitals NHS Foundation Trust Young Persons and Work Experience Students Under 18 Years of Age Policy Version No: 4.2 Effective From: 4 April 2016 Expiry Date: 4 April 2019 Date
Workforce Equality and Diversity Policy
 Type of Document Code: Policy Sponsor Lead Executive Recommended by: Workforce Equality and Diversity Policy Policy STHK0088 Deputy Human Resources Director Human Resources Director Policy Sub-Group Date
Type of Document Code: Policy Sponsor Lead Executive Recommended by: Workforce Equality and Diversity Policy Policy STHK0088 Deputy Human Resources Director Human Resources Director Policy Sub-Group Date
Document Title: Annual Progress Reports (APRs) Document Number: 056
 Document Number: 056") Document Title: Annual Progress Reports (APRs) Document Number: 056 Version: 1 Ratified by: Committee Date ratified: 30/11/2017 Name of originator/author: Directorate: Department: Name of responsible individual:
Document Title: Annual Progress Reports (APRs) Document Number: 056 Version: 1 Ratified by: Committee Date ratified: 30/11/2017 Name of originator/author: Directorate: Department: Name of responsible individual:
POLICY DEVELOPMENT, APPROVAL AND
 POLICY DEVELOPMENT, APPROVAL AND IMPLEMENTATION POLICY Ratification Process Lead Author: Developed by: Associate Director of Corporate Affairs CCG Secretary Directorate of Corporate Affairs Approved by:
POLICY DEVELOPMENT, APPROVAL AND IMPLEMENTATION POLICY Ratification Process Lead Author: Developed by: Associate Director of Corporate Affairs CCG Secretary Directorate of Corporate Affairs Approved by:
Additional Annual Leave Purchase Scheme V3.0
 Additional Annual Leave Purchase Scheme V3.0 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities...
Additional Annual Leave Purchase Scheme V3.0 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities...
Date ratified June, Implementation Date August, Date of full Implementation August, Review Date Feb, Version number V02.
 Document Title Reference Number Lead Officer Author(s) Ratified by Disputes Policy NTW(HR)07 Lisa Crichton-Jones Acting Executive Director of Workforce and Organisational Development Jacqueline Tate-Workforce
Document Title Reference Number Lead Officer Author(s) Ratified by Disputes Policy NTW(HR)07 Lisa Crichton-Jones Acting Executive Director of Workforce and Organisational Development Jacqueline Tate-Workforce
Lead Employer Annual Leave Policy. VERSION V11 January 2018
 Type of Document Code Policy Sponsor Lead Executive Recommended by VERSION V11 January 2018 Policy Deputy Director of HR Director of HR LNC Date Recommended 11 January 2018 Approved by Workforce Council
Type of Document Code Policy Sponsor Lead Executive Recommended by VERSION V11 January 2018 Policy Deputy Director of HR Director of HR LNC Date Recommended 11 January 2018 Approved by Workforce Council
This Policy supersedes the following Policy which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Environmental Sustainability Policy NTW(O)02 Paul McCabe, Head of Estates and Facilities (NTW Solutions Ltd) Sarah
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Environmental Sustainability Policy NTW(O)02 Paul McCabe, Head of Estates and Facilities (NTW Solutions Ltd) Sarah
Policy for the Development, Approval, Management and Dissemination of Trust Controlled Documents
 J Policy for the Development, Approval, Management and Dissemination of Trust Controlled Documents Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 55 6
J Policy for the Development, Approval, Management and Dissemination of Trust Controlled Documents Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 55 6
Lead Employer Flexible Working Policy. Trust Policy
 Lead Employer Flexible Working Policy Type of Document Code: Policy Sponsor Lead Executive Recommended by: Trust Policy Deputy Director of Human Resources Director of Human Resources Date Recommended:
Lead Employer Flexible Working Policy Type of Document Code: Policy Sponsor Lead Executive Recommended by: Trust Policy Deputy Director of Human Resources Director of Human Resources Date Recommended:
POLICY ON PROCEDURAL DOCUMENTS
 POLICY ON PROCEDURAL DOCUMENTS Policy Title: Executive Summary: Policy on Procedural Documents This policy provides guidance to authors of policies and procedures and staff in the Trust regarding the template
POLICY ON PROCEDURAL DOCUMENTS Policy Title: Executive Summary: Policy on Procedural Documents This policy provides guidance to authors of policies and procedures and staff in the Trust regarding the template
Performance and Development Review (PDR) Policy
 Policy") Performance and Development Review (PDR) Policy This Policy describes the process for undertaking a mandatory annual Performance and Development Review. Key Words: Performance, Development, Review Appraisal,
Performance and Development Review (PDR) Policy This Policy describes the process for undertaking a mandatory annual Performance and Development Review. Key Words: Performance, Development, Review Appraisal,
Directorate of Finance, Information & Performance Management DATA QUALITY POLICY
 Directorate of Finance, Information & Performance Management DATA QUALITY POLICY Reference: FPP003 Version: 1.5 This version issued: 10/03/11 Result of last review: Minor changes Date approved: 21/01/11
Directorate of Finance, Information & Performance Management DATA QUALITY POLICY Reference: FPP003 Version: 1.5 This version issued: 10/03/11 Result of last review: Minor changes Date approved: 21/01/11
Framework for Document Development
 Framework for Document Development Including the Production and Dissemination of Strategies, Policies, Procedures, Protocols and Guidelines Date: May 2011 Version number: 5 Author: Carolyn Hand, Corporate
Framework for Document Development Including the Production and Dissemination of Strategies, Policies, Procedures, Protocols and Guidelines Date: May 2011 Version number: 5 Author: Carolyn Hand, Corporate
Executive Director of Workforce and Organisational Development. Workforce Projects Manager. Date ratified January Implementation Date
 Document Title Reference Number Lead Officer Author(s) Ratified by Induction Policy NTW(HR)01 Lisa Crichton-Jones Executive Director of Workforce and Organisational Development Jacqueline Tate Workforce
Document Title Reference Number Lead Officer Author(s) Ratified by Induction Policy NTW(HR)01 Lisa Crichton-Jones Executive Director of Workforce and Organisational Development Jacqueline Tate Workforce
Lisa Quinn Executive Director of Performance and Assurance. Lead Officer
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Data Quality Policy NTW(O)26 Lisa Quinn Executive Director of Performance and Assurance Jennifer Illingworth Deputy
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Data Quality Policy NTW(O)26 Lisa Quinn Executive Director of Performance and Assurance Jennifer Illingworth Deputy
Appraisal Policy. Policy number:
 Appraisal Policy Policy number: HR10 Version: 3.0 Name of originator/author: Alison McQuillan Approving Committee Remuneration & Nominations Committee Date agreed 27 th May 2016 Next review date 27 th
Appraisal Policy Policy number: HR10 Version: 3.0 Name of originator/author: Alison McQuillan Approving Committee Remuneration & Nominations Committee Date agreed 27 th May 2016 Next review date 27 th
Unique Identifier: Document Type: POLICY Title: Corporate and Local Induction CORP/POL/045
 Document Type: POLICY Title: Corporate and Local Induction Target Audience: Trust Wide Author / Originator and Job Title: Vicki Wainwright, Compliance Replaces: Version 8 Corporate and Local Induction
Document Type: POLICY Title: Corporate and Local Induction Target Audience: Trust Wide Author / Originator and Job Title: Vicki Wainwright, Compliance Replaces: Version 8 Corporate and Local Induction
Type of Change. V01 New Mar 16 New Documentation. This Policy supersedes the following Policy which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Study Leave Policy for Medical Staff (Consultants and Specialty Doctors) NTW(HR)22 Rajesh Nadkarni Executive Medical
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Study Leave Policy for Medical Staff (Consultants and Specialty Doctors) NTW(HR)22 Rajesh Nadkarni Executive Medical
Development and Management of Procedural Documents
 Development and Management of Procedural Documents Target Audience Who Should Read This Policy Policy Leads/Authors Corporate Governance Staff Executive Directors Version 2.0 January 2015 Ref. Contents
Development and Management of Procedural Documents Target Audience Who Should Read This Policy Policy Leads/Authors Corporate Governance Staff Executive Directors Version 2.0 January 2015 Ref. Contents
Executive Director of Nursing and Chief Operating Officer. Lead Officer. Tony Gray Head of Safety, Security and Resilience
 Document Title Security Management Policy Reference Number Lead Officer Executive Director of Nursing and Chief Operating Officer Author(s) (name and designation) Ratified By: Tony Gray Head of Safety,
Document Title Security Management Policy Reference Number Lead Officer Executive Director of Nursing and Chief Operating Officer Author(s) (name and designation) Ratified By: Tony Gray Head of Safety,
Grievance Policy and Procedure
 Grievance Policy and Procedure Policy: HR03 Version: 2 Ratified by: Executive Management Team Date ratified: 13/10/2010 Name of originator/author: Andrew Stewart Name of responsible Senior HR Advisor,
Grievance Policy and Procedure Policy: HR03 Version: 2 Ratified by: Executive Management Team Date ratified: 13/10/2010 Name of originator/author: Andrew Stewart Name of responsible Senior HR Advisor,
Reference Check Completed by Joanne Shawcross..Date
 Document Type: Policy Document Title: Data Quality Scope: Trust Wide Author / Title: Rob O Neill, Information Manager Replaces: Information Assurance Strategy Validated By: Fiona Prestwood, Information
Document Type: Policy Document Title: Data Quality Scope: Trust Wide Author / Title: Rob O Neill, Information Manager Replaces: Information Assurance Strategy Validated By: Fiona Prestwood, Information
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Business Continuity Management Policy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Version No: 4.0 Effective From: 02 December 2016 Expiry Date: 02 December 2019 Date Ratified: 27 October 2016 Ratified by: Clinical Policy Group 1
The Newcastle upon Tyne Hospitals NHS Foundation Trust Version No: 4.0 Effective From: 02 December 2016 Expiry Date: 02 December 2019 Date Ratified: 27 October 2016 Ratified by: Clinical Policy Group 1
POLICY DEVELOPMENT FRAMEWORK
 POLICY DEVELOPMENT FRAMEWORK Lead Manager: Head of Policy Responsible Director: Director of Corporate Planning and Policy Approved by: Policy Planning and Performance Group Date approved: 17 January 2008
POLICY DEVELOPMENT FRAMEWORK Lead Manager: Head of Policy Responsible Director: Director of Corporate Planning and Policy Approved by: Policy Planning and Performance Group Date approved: 17 January 2008
POLICY FOR THE DEVELOPMENT, APPROVAL AND MANAGEMENT OF POLICIES
 POLICY FOR THE DEVELOPMENT, APPROVAL AND MANAGEMENT OF POLICIES Reference SWBH/ORG/011 Category Organisational Date Approved 27-08-2009 Date of Next Review 27-08-2011 Overview Key overall purpose of policy
POLICY FOR THE DEVELOPMENT, APPROVAL AND MANAGEMENT OF POLICIES Reference SWBH/ORG/011 Category Organisational Date Approved 27-08-2009 Date of Next Review 27-08-2011 Overview Key overall purpose of policy
Study Leave Policy for Senior Medical and Dental Staff
 Study Leave Policy for Senior Medical and Dental Staff Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that they should always refer to the Intranet
Study Leave Policy for Senior Medical and Dental Staff Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that they should always refer to the Intranet
Policies, Procedures, Guidelines and Protocols
 Policies, Procedures, Guidelines and Protocols Document Details Title Policy on the Development and Management of Procedural Documents (Strategies, Policies, Protocols and Guidelines) Trust Ref No 1361-28127
Policies, Procedures, Guidelines and Protocols Document Details Title Policy on the Development and Management of Procedural Documents (Strategies, Policies, Protocols and Guidelines) Trust Ref No 1361-28127
JOB SHARE POLICY AND PROCEDURES JANUARY This policy supersedes all previous policies for Job Share Policy and Procedures
 JOB SHARE POLICY AND PROCEDURES JANUARY 2016 This policy supersedes all previous policies for Job Share Policy and Procedures JOB SHARE POLICY_HR24_JANUARY 2016 Policy title Job Share Policy and Procedures
JOB SHARE POLICY AND PROCEDURES JANUARY 2016 This policy supersedes all previous policies for Job Share Policy and Procedures JOB SHARE POLICY_HR24_JANUARY 2016 Policy title Job Share Policy and Procedures
Policy for Equality and Diversity
 Policy for Equality and Diversity HR01 Related Policies: HR07 Disciplinary Procedure for Doctors and Dentists HR16 Disputes and Grievances HR29 Time off for Special Circumstances HR33 Recruitment & Selection
Policy for Equality and Diversity HR01 Related Policies: HR07 Disciplinary Procedure for Doctors and Dentists HR16 Disputes and Grievances HR29 Time off for Special Circumstances HR33 Recruitment & Selection
Planned and Reactive Maintenance Policy V1.1
 V1.1 November 2016 Summary Page 2 of 15 Table of Contents 1. Introduction... 4 2. Purpose of this Policy/Procedure... 4 3. Scope... 4 4. Definitions / Glossary... 4 5. Ownership and Responsibilities...
V1.1 November 2016 Summary Page 2 of 15 Table of Contents 1. Introduction... 4 2. Purpose of this Policy/Procedure... 4 3. Scope... 4 4. Definitions / Glossary... 4 5. Ownership and Responsibilities...
INFORMATION GOVERNANCE POLICY
 INFORMATION GOVERNANCE POLICY Unique Reference / Version Primary Intranet Location Information Management & Governance Secondary Intranet Location Policy Name Information Governance Policy Version Number
INFORMATION GOVERNANCE POLICY Unique Reference / Version Primary Intranet Location Information Management & Governance Secondary Intranet Location Policy Name Information Governance Policy Version Number
Learning and development policy. Document author Assured by Review cycle. 1. Introduction Policy statement Purpose or aim...
 Learning and development policy Board library reference Document author Assured by Review cycle P090 Head of Learning and Development Quality and Standards Committee 3 years This document is version controlled.
Learning and development policy Board library reference Document author Assured by Review cycle P090 Head of Learning and Development Quality and Standards Committee 3 years This document is version controlled.
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Employment Policies and Procedures
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Recognition Agreement for Trade Unions/Professional Staff Organisations Version.: 7 Effective Date: 17 December
The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Recognition Agreement for Trade Unions/Professional Staff Organisations Version.: 7 Effective Date: 17 December
Policy and Procedure in case of an under or overpayment of salary, allowances and benefits. V4.0
 Policy and Procedure in case of an under or overpayment of salary, allowances and benefits. V4.0 Summary. The Trust has a duty to ensure that all staff are paid correctly. Occasionally, there will be incorrect
Policy and Procedure in case of an under or overpayment of salary, allowances and benefits. V4.0 Summary. The Trust has a duty to ensure that all staff are paid correctly. Occasionally, there will be incorrect
Equality and Diversity Policy
 Equality and Diversity Policy Author(s) (name and post): Version No.: Version 2 Lisa Kelly, HR Business Partner, MLCSU Approval Date: 21 st November 2017 Review Date: July 2021 Author/s: NHS Staffordshire
Equality and Diversity Policy Author(s) (name and post): Version No.: Version 2 Lisa Kelly, HR Business Partner, MLCSU Approval Date: 21 st November 2017 Review Date: July 2021 Author/s: NHS Staffordshire
Pay Protection Policy V2.0
 V2.0 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 4 5.1. Role of the Chief Executive...
V2.0 Table of Contents 1. Introduction... 3 2. Purpose of this Policy/Procedure... 3 3. Scope... 3 4. Definitions / Glossary... 3 5. Ownership and Responsibilities... 4 5.1. Role of the Chief Executive...
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Employment Policies and Procedures. Electronic Rostering and Attendance (ERA)
") The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Electronic Rostering and Attendance (ERA) Version No.: 4.0 Effective Date: 23 January 2017 Expiry Date: 23 January
The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Electronic Rostering and Attendance (ERA) Version No.: 4.0 Effective Date: 23 January 2017 Expiry Date: 23 January
Induction Policy. Document author Assured by Review cycle. 1. Introduction Policy Statement Purpose or Aim Scope...
 Induction Policy Board library reference Document author Assured by Review cycle P091 Head of Learning and Development Quality and Standards Committee 3 Year This document is version controlled. The master
Induction Policy Board library reference Document author Assured by Review cycle P091 Head of Learning and Development Quality and Standards Committee 3 Year This document is version controlled. The master
Colchester Hospital University NHS Foundation Trust. Equality Act Equality Delivery System Equality Objectives April March 2016
 Introduction Colchester Hospital University NHS Foundation Trust Equality Act Equality Delivery System Equality Objectives April 2012 - March 2016 The Public Sector Equality Duties require that public
Introduction Colchester Hospital University NHS Foundation Trust Equality Act Equality Delivery System Equality Objectives April 2012 - March 2016 The Public Sector Equality Duties require that public
GRIEVANCE POLICY AND PROCEDURE Dealing with Employee Concerns
 GRIEVANCE POLICY AND PROCEDURE Dealing with Employee Concerns Responsible Approved By Equality Assessed of Human Resources Area Partnership Forum We are working to ensure that no-one is treated in an unlawful
GRIEVANCE POLICY AND PROCEDURE Dealing with Employee Concerns Responsible Approved By Equality Assessed of Human Resources Area Partnership Forum We are working to ensure that no-one is treated in an unlawful
DOCUMENT CONTROL PAGE. Health and Safety Policy Statement
 Review Circulation Application Ratification Originator or modifier Minor Amendment Supersedes Title DOCUMENT CONTROL PAGE Title: Health and Safety Policy Statement Version: 5.0 Reference Number: HSP 1
Review Circulation Application Ratification Originator or modifier Minor Amendment Supersedes Title DOCUMENT CONTROL PAGE Title: Health and Safety Policy Statement Version: 5.0 Reference Number: HSP 1
The Health Board objective of delivering the highest quality services possible can only be achieved by a workforce that is sufficiently skilled,
 Section A: Assessment Name of Policy Partnership and Recognition Agreement Person/persons conducting this assessment with Contact Details Rachel Pressley, Workforce Governance Manager Andrew Crook, Head
Section A: Assessment Name of Policy Partnership and Recognition Agreement Person/persons conducting this assessment with Contact Details Rachel Pressley, Workforce Governance Manager Andrew Crook, Head
CONDUCTING PERSONAL APPRAISAL DEVELOPMENT REVIEWS (PADRs) POLICY
 POLICY") AGENDA ITEM 4.2 Appendix a CONDUCTING PERSONAL APPRAISAL DEVELOPMENT REVIEWS (PADRs) POLICY Reference No: UHB 079 Version No: 1 Previous Trust / LHB Ref No: T193 Documents to read alongside this Policy
AGENDA ITEM 4.2 Appendix a CONDUCTING PERSONAL APPRAISAL DEVELOPMENT REVIEWS (PADRs) POLICY Reference No: UHB 079 Version No: 1 Previous Trust / LHB Ref No: T193 Documents to read alongside this Policy
Asbestos Management Plan. Policy, Organisation and Arrangements V2.2
 Asbestos Management Plan Policy, Organisation and Arrangements V2.2 December 2015 Summary / Policy Statement The Royal Cornwall Hospitals NHS Trust is committed to meeting all the duties placed upon it
Asbestos Management Plan Policy, Organisation and Arrangements V2.2 December 2015 Summary / Policy Statement The Royal Cornwall Hospitals NHS Trust is committed to meeting all the duties placed upon it
Equality and Diversity Policy
 Equality and Diversity Policy Hertfordshire, Bedfordshire and Luton Clinical Commissioning Groups Page 1 of 15 DOCUMENT CONTROL SHEET Document Owner: Director of Workforce Document Author(s): Louise Thomas,
Equality and Diversity Policy Hertfordshire, Bedfordshire and Luton Clinical Commissioning Groups Page 1 of 15 DOCUMENT CONTROL SHEET Document Owner: Director of Workforce Document Author(s): Louise Thomas,
SOMERSET PARTNERSHIP NHS FOUNDATION TRUST STRENGTHENING GOVERNANCE ARRANGEMENTS. Report to the Trust Board 24 May 2016
 R SOMERSET PARTNERSHIP NHS FOUNDATION TRUST STRENGTHENING GOVERNANCE ARRANGEMENTS Report to the Trust Board 24 May 2016 Sponsoring Director: Author: Purpose of the report: Key Issues and Recommendations:
R SOMERSET PARTNERSHIP NHS FOUNDATION TRUST STRENGTHENING GOVERNANCE ARRANGEMENTS Report to the Trust Board 24 May 2016 Sponsoring Director: Author: Purpose of the report: Key Issues and Recommendations:
Controlled Document Number: Version Number: 002. On: October Review Date: October 2020 Distribution: Essential Reading for: Page 1 of 12
 Equality and Diversity in Employment Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Version Number: 002 Controlled Document Sponsor: Controlled Document
Equality and Diversity in Employment Policy CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Policy Version Number: 002 Controlled Document Sponsor: Controlled Document
Corporate Document Approval Framework
 Corporate Document Approval Framework Author(s) (name and post): Lezli Feeney, Risk Manager Alan Ferguson, Records Manager Version No.: Version 1.2 Approval Date: 18 Jan 2011 Review Date: 17 Jan 2013 the
Corporate Document Approval Framework Author(s) (name and post): Lezli Feeney, Risk Manager Alan Ferguson, Records Manager Version No.: Version 1.2 Approval Date: 18 Jan 2011 Review Date: 17 Jan 2013 the
Capability Policy and Procedure
 Capability Policy and Procedure Version 2.4 Important: This document can only be considered valid when viewed on the Trust Website. If this document has been printed or saved to another location, you must
Capability Policy and Procedure Version 2.4 Important: This document can only be considered valid when viewed on the Trust Website. If this document has been printed or saved to another location, you must
IGPr002 - Information Governance Management Framework
 IGPr002 - Information Governance Management Framework Page 1 of 10 Table of Contents Information Governance Management Framework... 1 Why we need this Framework... 3 What the Framework is trying to do...
IGPr002 - Information Governance Management Framework Page 1 of 10 Table of Contents Information Governance Management Framework... 1 Why we need this Framework... 3 What the Framework is trying to do...
NHS Lewisham CCG Grievance Policy & Procedure
 NHS Lewisham CCG Grievance Policy & Procedure 1 CCG Policy Reference: This policy replaces or supersedes Policy Ref: Target Audience Brief Description (max 50 words) Action Required Governing Body members,
NHS Lewisham CCG Grievance Policy & Procedure 1 CCG Policy Reference: This policy replaces or supersedes Policy Ref: Target Audience Brief Description (max 50 words) Action Required Governing Body members,
DATA QUALITY POLICY. Ref No:
 Ref No: DATA QUALITY POLICY Version: 4e Ratified by: Policy Ratification Group Date ratified: 15 December 2010 Name of author: Head of Information & Performance Name of responsible committee: Quality Committee
Ref No: DATA QUALITY POLICY Version: 4e Ratified by: Policy Ratification Group Date ratified: 15 December 2010 Name of author: Head of Information & Performance Name of responsible committee: Quality Committee
62 GB Long Service and Achievement Awards Policy
 62 GB Long Service and Achievement Awards Policy Policy number Version 3.0 Approved by Name of author/originator Owner (director) 62 GB Governing Body Date of approval April 2017 Date of last review March
62 GB Long Service and Achievement Awards Policy Policy number Version 3.0 Approved by Name of author/originator Owner (director) 62 GB Governing Body Date of approval April 2017 Date of last review March
POLICY FOR THE MANAGEMENT OF POLICIES AND STANDARD OPERATING PROCEDURES
 POLICY FOR THE MANAGEMENT OF POLICIES AND STANDARD OPERATING PROCEDURES Subject and version number of document: Serial Number: Policy for the Management of Policies and V2 PFMPV2 Operative date: 1 April
POLICY FOR THE MANAGEMENT OF POLICIES AND STANDARD OPERATING PROCEDURES Subject and version number of document: Serial Number: Policy for the Management of Policies and V2 PFMPV2 Operative date: 1 April
Suspension, Exclusion or Transfer Policy
 Suspension, Exclusion or Transfer Policy Solent NHS Trust Policies can only be considered to be valid and up-to-date if viewed on the intranet. Please visit the intranet for the latest version. Purpose
Suspension, Exclusion or Transfer Policy Solent NHS Trust Policies can only be considered to be valid and up-to-date if viewed on the intranet. Please visit the intranet for the latest version. Purpose
R&D Administration Manager. Research and Development. Research and Development
 Document Title: Document Number: Trial Closure and End of Trial SOP021 Staff involved in development: Job titles only Document author/owner: Directorate: Department: For use by: RM&G Manager, R&D Administration
Document Title: Document Number: Trial Closure and End of Trial SOP021 Staff involved in development: Job titles only Document author/owner: Directorate: Department: For use by: RM&G Manager, R&D Administration
Moving and Handling Policy
 Moving and Handling Policy Ratified Governance and Risk Committee Status Approved Issued August 2014 Approved By Governance and Risk Committee Consultation Governance and Risk Committee Equality
Moving and Handling Policy Ratified Governance and Risk Committee Status Approved Issued August 2014 Approved By Governance and Risk Committee Consultation Governance and Risk Committee Equality
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Employment Policies and Procedures
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Safeguarding Adults Guidance on Handling Allegations/Complaints of Abuse Made Against Employees Version No: 3.1
The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Safeguarding Adults Guidance on Handling Allegations/Complaints of Abuse Made Against Employees Version No: 3.1
Provision of Use of Work Equipment Policy
 Provision of Use of Work Equipment Policy Ratified Status Approved Approved Issued March 2017 Approved By Consultation Equality Impact Assessment Formal Executive Team CCG Corporate Governance & Risk Manager
Provision of Use of Work Equipment Policy Ratified Status Approved Approved Issued March 2017 Approved By Consultation Equality Impact Assessment Formal Executive Team CCG Corporate Governance & Risk Manager
Ethical Approval. Document Number: 012
 Ethical Approval Document Number: 012 Version: 1 Ratified by: RFL Committee Date ratified: 03.06.2014 Name of originator/author: Directorate: Department: Name of responsible individual: Liba Stones, Manager
Ethical Approval Document Number: 012 Version: 1 Ratified by: RFL Committee Date ratified: 03.06.2014 Name of originator/author: Directorate: Department: Name of responsible individual: Liba Stones, Manager
Directorate of Strategy & Planning DATA QUALITY POLICY
 Directorate of Strategy & Planning DATA QUALITY POLICY Reference: FPP003 Version: 1.6 This version issued: 24/06/14 Result of last review: Minor changes Date approved by owner (if applicable): N/A Date
Directorate of Strategy & Planning DATA QUALITY POLICY Reference: FPP003 Version: 1.6 This version issued: 24/06/14 Result of last review: Minor changes Date approved by owner (if applicable): N/A Date
SINGLE EQUALITY POLICY
 SINGLE EQUALITY POLICY 1 CONTENTS A: POLICY 1. Introduction Page 3 2. College Values Page 3 3. Legal Framework Page 4 4. Scope Page 4 5. Structures Page 4 6. Monitoring Page 5 7. Reporting Page 5 8. Positive
SINGLE EQUALITY POLICY 1 CONTENTS A: POLICY 1. Introduction Page 3 2. College Values Page 3 3. Legal Framework Page 4 4. Scope Page 4 5. Structures Page 4 6. Monitoring Page 5 7. Reporting Page 5 8. Positive
INFORMATION GOVERNANCE STRATEGY AND STRATEGIC VISION
 INFORMATION GOVERNANCE STRATEGY AND STRATEGIC VISION Policy approved by: Joint Audit and Governance Committee Date: December 2016 Next Review Date: October 2018 Version: 2.0 Information Governance Strategy
INFORMATION GOVERNANCE STRATEGY AND STRATEGIC VISION Policy approved by: Joint Audit and Governance Committee Date: December 2016 Next Review Date: October 2018 Version: 2.0 Information Governance Strategy
Equal Opportunities in Employment
 Equal Opportunities in Employment Keywords: Equal Opportunities, Employment Document No: EDH004 Version: 5.1 Developed in Consultation with: Central Policy Group Ratified by: CJNCC Executive Directors
Equal Opportunities in Employment Keywords: Equal Opportunities, Employment Document No: EDH004 Version: 5.1 Developed in Consultation with: Central Policy Group Ratified by: CJNCC Executive Directors
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Employment Policies and Procedures
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Safeguarding Adults Guidance on Handling Allegations/Complaints of Abuse Made Against Employees Version No: 2.1
The Newcastle upon Tyne Hospitals NHS Foundation Trust Employment Policies and Procedures Safeguarding Adults Guidance on Handling Allegations/Complaints of Abuse Made Against Employees Version No: 2.1
HONORARY EMERITUS STATUS FOR RETIRING CONSULTANT STAFF (MD10)
") HONORARY EMERITUS STATUS FOR RETIRING CONSULTANT STAFF (MD10) If you require a copy of this policy in an alternative format (for example large print, easy read) or would like any assistance in relation
HONORARY EMERITUS STATUS FOR RETIRING CONSULTANT STAFF (MD10) If you require a copy of this policy in an alternative format (for example large print, easy read) or would like any assistance in relation
Risk Assessment Procedure
 Risk Assessment Procedure Version: 1.1 Ratified by (Committee) : EMG Date ratified: 06.05.14 Name of originator/author: Developed in association with: Catherine McGowan Workplace Law Name of executive
Risk Assessment Procedure Version: 1.1 Ratified by (Committee) : EMG Date ratified: 06.05.14 Name of originator/author: Developed in association with: Catherine McGowan Workplace Law Name of executive
Trust Policy Supply Chain Inventory Management Policy (SC010)
") Trust Policy Supply Chain Inventory Management Policy (SC010) Purpose Date Version 16/09/16 1 The purpose of this Supply Chain Inventory Management Policy is to identify the relevant Standard Operating
Trust Policy Supply Chain Inventory Management Policy (SC010) Purpose Date Version 16/09/16 1 The purpose of this Supply Chain Inventory Management Policy is to identify the relevant Standard Operating
Equal Opportunities in Employment Policy
 1 Equal Opportunities in Employment Policy Version: 2 Policy Lead: Policy Category: Louise rris Human Resources Date issued: October 2010 Review date: October 2013 Ratified by: Governance Executive Date
1 Equal Opportunities in Employment Policy Version: 2 Policy Lead: Policy Category: Louise rris Human Resources Date issued: October 2010 Review date: October 2013 Ratified by: Governance Executive Date
Managing Work Performance Policy
 MWP001 April 2014 Managing Work Performance Policy Policy Number Target Audience Approving Committee MWP001 CCG staff CCG Executive Date Approved 9 th April 2014 Last Review Date April 2014 Next Review
MWP001 April 2014 Managing Work Performance Policy Policy Number Target Audience Approving Committee MWP001 CCG staff CCG Executive Date Approved 9 th April 2014 Last Review Date April 2014 Next Review
Trust Policy Policy for the Award of Honorary Contracts for Retired Senior Medical and Dental Staff
 Trust Policy Policy for the Award of Honorary Contracts for Retired Senior Medical and Dental Purpose Date Version April 2015 6 To set out the key elements which the Trust will apply when considering whether
Trust Policy Policy for the Award of Honorary Contracts for Retired Senior Medical and Dental Purpose Date Version April 2015 6 To set out the key elements which the Trust will apply when considering whether
AGENDA FOR CHANGE JOB MATCHING AND JOB EVALUATION PROCEDURE
 AGENDA FOR CHANGE JOB MATCHING AND JOB EVALUATION PROCEDURE Document Summary This procedure supports the practice of equal pay for work of equal value within Cumbria Partnership NHS Foundation Trust, in
AGENDA FOR CHANGE JOB MATCHING AND JOB EVALUATION PROCEDURE Document Summary This procedure supports the practice of equal pay for work of equal value within Cumbria Partnership NHS Foundation Trust, in
CCG CO 22 Project Management Policy
 Corporate CCG CO 22 Project Management Policy Version Number Date Issued Review Date V1.1 25/02/2016 25/02/2018 Prepared By: Head of Programme Management Office (PMO), NTCCG Consultation Process: Transformation
Corporate CCG CO 22 Project Management Policy Version Number Date Issued Review Date V1.1 25/02/2016 25/02/2018 Prepared By: Head of Programme Management Office (PMO), NTCCG Consultation Process: Transformation
Author s job title Head of Clinical Coding and Data Quality Directorate IM&T
 Document Control Title Data Quality Policy Author Author s job title Head of Clinical Coding and Data Quality Directorate IM&T Department Clinical Coding Version Date Issued Status Comment / Changes /
Document Control Title Data Quality Policy Author Author s job title Head of Clinical Coding and Data Quality Directorate IM&T Department Clinical Coding Version Date Issued Status Comment / Changes /
Capability Policy. Human Resources Business Partner Version nd July Greenwich Executive Group
 Capability Policy Author(s) Human Resources Business Partner Version 0.1 Version Date 2 nd May 2014 Implementation/Approval Date 2 nd July 2014 Review Date July 2017 Review Body Greenwich Executive Group
Capability Policy Author(s) Human Resources Business Partner Version 0.1 Version Date 2 nd May 2014 Implementation/Approval Date 2 nd July 2014 Review Date July 2017 Review Body Greenwich Executive Group
Equality and Diversity policy
 Equality and Diversity policy Document Reference No. KCHFT HR012 Status Final Version Number 2.5 Replacing/Superseded policy or Equality and Diversity Policy v2.4 documents Number of Pages 13 Target audience/applicable
Equality and Diversity policy Document Reference No. KCHFT HR012 Status Final Version Number 2.5 Replacing/Superseded policy or Equality and Diversity Policy v2.4 documents Number of Pages 13 Target audience/applicable
Equality & Diversity Policy HR 19
 ESTUARY HOUSING ASSOCIATION LTD DIRECTORATE / DEPARTMENT: Human Resources AUTHOR: Linda Hollingworth Assistant Director of Human Resources & Organisational Development Committee: Corporate Health & Remuneration
ESTUARY HOUSING ASSOCIATION LTD DIRECTORATE / DEPARTMENT: Human Resources AUTHOR: Linda Hollingworth Assistant Director of Human Resources & Organisational Development Committee: Corporate Health & Remuneration
Standards of proficiency. Biomedical scientists
 Standards of proficiency Biomedical scientists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of proficiency
Standards of proficiency Biomedical scientists Contents Foreword 1 Introduction 3 Standards of proficiency 7 Foreword We are pleased to present the Health and Care Professions Council s standards of proficiency
CCG CO 22 Project Management Policy
 Corporate CCG CO 22 Project Management Policy Version Number Date Issued Review Date V2.0 20/05/2016 20/05/2018 Prepared By: Head of Programme Management Office (PMO), NTCCG Consultation Process: Transformation
Corporate CCG CO 22 Project Management Policy Version Number Date Issued Review Date V2.0 20/05/2016 20/05/2018 Prepared By: Head of Programme Management Office (PMO), NTCCG Consultation Process: Transformation